Distribution in nature
Minerals that contain magnesium hydroxide are quite rare. Among these minerals, brucite is the most important. In addition to the main compound, Mg (OH) 2, it may contain impurities MnO, FeO, Fe 2 O 3. Brucite is formed as a result of the hydrolysis of natural magnesium compounds soluble in meadows.
Mg (OH) 2 is also found in the mineral hydromagnesite, which in composition is close to a mixture of magnesium hydroxide and carbonate - 4MgCO 3 Mg (OH) 2 2H 2 O.
Receipt
Given the low prevalence of magnesium hydroxide in mineral deposits, it is mined using a different method. For industrial needs, Mg (OH) 2 is obtained by precipitation of sea water and brines. Hydroxide extraction from sea water was first used in 1865 on the French Mediterranean coast.
In laboratory languages, magnesium hydroxide can be synthesized by burning magnesium metal in water vapor:
Precipitation of poorly soluble hydroxide during the interaction of magnesium salts with alkalis and ammonium hydroxide is also used.
However, precipitation with ammonium hydroxide occurs entirely due to the constant decrease in OH - ions.
Oral Bioavailability of Magnesium Oxide and Other Compounds (Review)
To date, there is no accurate data on the superiority of one or another magnesium preparation for oral use. Gastrointestinal absorption and other pharmacokinetic parameters of oral magnesium compounds are key to predicting the effectiveness of these drugs as a source of magnesium.
There is a widespread belief that organic magnesium compounds are better absorbed from the gastrointestinal tract than inorganic ones [1–3], however, the results of studies do not always confirm this point of view [4, 5], and the confirmatory ones are sometimes carried out not entirely correctly. For example, in a domestic study, the dynamics of magnesium concentration in blood plasma and erythrocytes was studied after a single administration of various dosage forms of magnesium preparations. The study had a cross-sectional design. 16 volunteers (11 men and 5 women) took part in it. Volunteers participated in the experiment repeatedly; between studies with the participation of the same volunteer, a gap of at least 15 days was maintained. Participants received Magne B6 8 tablets (Mg lactate dihydrate + pyridoxine, 384 mg based on pure Mg), Magne B6 3 ampoules (Mg lactate dihydrate + Mg pidolate + pyridoxine, 300 mg Mg). The comparison drug Berocca Plus was prescribed, according to the instructions, 1 tablet per day (Mg sulfate and carbonate, 100 mg Mg). Bioavailability was assessed as the area under the curve in plasma and erythrocytes. The differences in bioavailability between Magne B6 preparations and the control were statistically significant. The authors note a significantly higher bioavailability of organic magnesium in the form of both forms of Magne B6 compared to the reference drug, Berocca Plus. It is surprising that the authors compare the areas under the curve of drugs in which the magnesium content differs by at least 3 times [6].
It should be noted that, despite the active interest in the role of magnesium in metabolic processes, the effect of magnesium deficiency on the development of neurological and cardiovascular pathology, pathology of pregnancy, etc., studies studying the pharmacokinetics of oral magnesium preparations, including its oxide is very small [1].
In 1973, DA Cook published the results of a large experimental study of the pharmacokinetics of oral inorganic magnesium compounds in rats. After 5 days, the animals received a low magnesium diet for 14 weeks. magnesium in the form of magnesium oxide or chloride, or carbonate, or bicarbonate, or phosphate, or sulfate or silicate, or remained on a depleted diet. After this, the animals were killed and the levels of calcium and magnesium in the femurs, kidneys, urine, plasma, excrement were analyzed using the spectrophotometric method, then the absorption of magnesium was calculated: for carbonate it turned out to be 64.9%; for chloride – 61%, for oxide – 58%, for phosphate – 54.1%, for sulfate – 53.3%, for silicate – 54.2% [7].
In 1990, JS Lindberg et al. conducted an in vitro and in vivo study to compare the oral absorption of magnesium oxide and citrate in humans. The solubility of 25 mmol of both substances in 300 ml of hydrochloric acid solutions of different concentrations (0–24.2 mEq) and distilled water was compared. Magnesium oxide is practically insoluble in water and only 43% soluble in the most concentrated acid solution. Magnesium citrate in distilled water had a solubility of 55% and was more soluble than the oxide in acidic solutions. When the pH of the solutions was restored to 7 by titration with bicarbonate, neither the citrate nor the oxide recrystallized. Healthy volunteers received 25 mmol of either citrate or magnesium oxide orally. The level of salt absorption was assessed by changes in urinary excretion of magnesium. The increase in urinary magnesium levels was significantly higher in the group of volunteers receiving citrate [8].
In 1990, T. Bohmer et al. published the results of a study of magnesium excretion in healthy young female volunteers (students) within 24 hours after administration of magnesium in the form of hydroxide, citrate, magnesium lactate or placebo 3 times/day in a daily dose of 15–20.6 mmol. All drugs significantly increased the level of urinary excretion of magnesium, but there were no statistical differences in urinary excretion between participants taking different magnesium drugs. However, it should be noted that only 18 people took part in the study [9].
In 1994, SA Schuette et al. published data from a study of the intestinal absorption of magnesium oxide and chelated magnesium diglycinate, labeled with the 26Mg isotope, in patients (12 people) who had undergone ileal resection. The study had a double-blind, crossover design, with a dose of 100 mg. Magnesium oxide and diglycinate showed bioavailability of 22.8 and 23.5%, respectively, but there was a trend toward higher absorption of diglycinate in the 4 patients in whom the oxide was the worst absorbed. In addition, the peak plasma concentration of the isotope after taking diglycinate occurred earlier by 3.2 ± 1.3 hours [10]. AF Walker et al. (2003) studied the comparative pharmacokinetics of magnesium compounds (oxide, citrate and magnesium amino acid chelate (AAC)) in healthy volunteers in a double-blind, randomized, placebo-controlled study. Volunteers without signs of magnesium deficiency were randomized into 5 groups: receiving magnesium oxide 300 mg/day; magnesium citrate – 300 mg/day; Mg AAS, as well as 2 placebo groups: one took cellulose, the other took sorbitol. The drugs were taken for 60 days, patients were examined after the first day of administration and after 60 days of therapy. We studied magnesium levels in the blood (plasma and red blood cells), urine and saliva using atomic absorption spectrophotometry. Interestingly, in all groups, the initial average plasma magnesium levels were below normal. In blood plasma, citrate was the most effective. It significantly increased magnesium levels compared to AAS after 60 days of therapy, but there was no statistical difference between the results in the citrate and oxide groups. In this study, only the citrate group had significantly increased salivary magnesium levels. There were no differences between groups in erythrocyte magnesium levels. The researchers note that theoretically, magnesium oxide should cause a laxative effect, but the experiment participants who received it did not note such an effect of the drug [11].
C. Coudray et al. (2005) used a series of tests to investigate the intestinal absorption and urinary elimination, as well as the accumulation of various magnesium compounds in the body of male Wistar rats. The rats received magnesium oxide or magnesium chloride or sulfate or carbonate or acetate or pidolate or gluconate or citrate or lactate or aspartate. Before the study for 3 weeks. The rats received a diet with a reduced magnesium content (150 mg/kg). Then the rats in all groups received the same amount of magnesium in the form of its various compounds (550 mg/kg body weight). The experiment was continued for up to 6 weeks, and then the animals were sacrificed and the magnesium content in plasma, red blood cells and bones was measured using a precise method - inductively coupled plasma mass spectrometry. Plasma levels of magnesium, its content in red blood cells and bones after the use of different salts did not show significant differences, with a tendency to superiority when using magnesium gluconate. Finally, fecal and urinary excretion of magnesium were examined and intestinal magnesium absorption was calculated. The results demonstrate the lag of inorganic magnesium compounds (among them, magnesium oxide and chloride are better absorbed - 48.4% and 48.8%, respectively, sulfate is the worst - only 34.8%), and among organic salts the record holder is again gluconate - 56.8% .
The authors conclude that with a slight superiority of organic magnesium compounds (especially magnesium gluconate) and a slight lag in magnesium sulfate, all magnesium compounds are able to be absorbed and affect its levels in the blood and tissues [5].
In 2006, the results of a domestic study were published in the journal “Nutrition Issues” [Konyukhova O.S. et al.] pharmacokinetics of magnesium preparations and vitamins, conducted with the participation of 60 volunteers, of whom 15 received magnesium-containing preparations Magnerot (500 mg magnesium orotate; in terms of Mg2+ - 32.8 mg) once orally and another 15 people received Centrum (100 magnesium oxide; in terms of Mg – 60.3 mg). Based on the results of the study, the authors note that when taking the studied magnesium preparations in the body, an equal increase in the concentration of this element occurs in the body, but when taking magnesium oxide, it occurs at a later date [4].
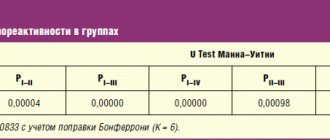
The purpose of the study conducted at the Volgograd State Medical University [Spasov A.A. et al., 2010], there was a comparison of the rate of compensation of nutritional magnesium deficiency (Mg after the introduction of 8 inorganic and 12 organic magnesium salts), as well as an assessment of the ability of vitamin B6 to accelerate compensation of magnesium deficiency when combined with magnesium salts. To develop magnesium deficiency, 280 rats received a magnesium-deficient diet (magnesium content no more than 15 mg/kg) and distilled water for 7 weeks. A group of intact rats (12 animals) received a magnesium-balanced diet (Mg content – 500 mg per 1 kg of diet). Starting from the 49th day of the diet, the animals received magnesium salts (Mg chloride, Mg sulfate, Mg oxide, Mg nitrate, Mg thiosulfate, Mg hydrogen phosphate, Mg carbonate, Mg trisilicate, Mg L-, D- and DL-aspartate, Mg L- , and DL-pyroglutamate, Mg succinate, Mg glycinate, Mg orotate, Mg taurine, Mg lactate) or their combination with vitamin B6 at a dose of 50 mg of elemental magnesium and 5 mg of vitamin B6 per 1 kg of body weight. It was found that magnesium L-aspartate most effectively and quickly compensates for magnesium deficiency compared to all other magnesium salts. Among inorganic magnesium salts, the leader in the rate of compensation of magnesium deficiency was chloride, and the effectiveness of chloride immediately followed L-aspartate, ahead of other organic and inorganic salts. The effectiveness of the oxide was not inferior to either lactate or magnesium orotate [13].
The study of the bioavailability of magnesium preparations when taken orally continues. In Israel at the Medical Center. Chaim Shiba recently conducted a comprehensive comparative study of two compounds: magnesium oxide and magnesium citrate. Under observation were 41 healthy volunteers who did not have diagnosed heart disease. They were randomly distributed into two groups. For one month, the subjects in each group received one of two drugs available on the Israeli pharmaceutical market: magnesium citrate under the commercial name Magnesium Diasporal (295.8 mg of magnesium in one tablet) or magnesium oxide monohydrate under the commercial name Magnox 520. At the end of this month there was also a break in taking the drugs for 1 month, after which, already on the 3rd month. study, volunteers began taking magnesium supplements again, but each volunteer was already receiving a second drug for him: that is, those who first received magnesium citrate, this time took magnesium oxide, and vice versa. Before the start of each monthly drug intake and upon its completion, a study of magnesium concentrations in the blood serum and in the tissue cells of the volunteer’s body was carried out, platelet activity and electrolyte concentrations in the blood serum were studied. Volunteers were asked to fill out questionnaires regarding the quality of their daily lives. It was found that taking magnesium oxide significantly increased the concentration of magnesium in the body's cells and led to a decrease in the concentrations of low-density cholesterol and C-reactive protein. At the same time, taking magnesium citrate did not lead to such positive changes in laboratory parameters. The functional activity of platelets improved under the influence of both drugs [14].
Thus, the results of the few pharmacokinetic studies that determine the characteristics of the absorption of various magnesium salts from the gastrointestinal tract demonstrate a number of factors that impede the study of intestinal absorption of magnesium preparations.
Most studies of the pharmacokinetics of magnesium compounds have consisted of studying the level of urinary excretion of magnesium during the day and/or the concentration of magnesium ions in plasma/serum, which makes it possible only for an approximate assessment of intestinal absorption of magnesium. It should be remembered that plasma magnesium levels are subject to homeostatic control and magnesium can easily be lost from plasma to organs and tissues, and that plasma concentration is not an accurate indicator of intestinal magnesium absorption. Moreover, serum magnesium levels can remain within normal limits even when the total amount of magnesium in the body decreases by 80% due to the release of the trace element from the depot [15]. It can be said that to date there is no single generally accepted method for studying the effect of magnesium preparations on its content in the human body, and this makes it very difficult to study any pharmacokinetic parameters of these compounds. In addition, the rather limited number of participants in studies of the pharmacokinetics of magnesium preparations in humans and conflicting results are noteworthy.
Some authors consider it most appropriate to study the level of magnesium in erythrocytes and/or lymphocytes, as well as its concentration in saliva, but there is no consensus on this issue [5, 16, 17].
Based on the mechanisms of magnesium absorption in the intestine (passive diffusion along the electrochemical concentration gradient), it can be assumed that the lower the solubility, the better the absorption in the gastrointestinal tract. But the results of comparative studies indicate that the outsider in terms of bioavailability is not magnesium oxide (which is practically insoluble), but sulfate, which has good solubility (33.7 g in 100 g of water at 20°C) [5, 13].
Magnesium oxide, like other magnesium compounds, in experimental studies has proven the ability to successfully relieve deficiency of this element. Unfortunately, the above difficulties in assessing the bioavailability of magnesium compounds hinder the development of methodology for such studies. It is especially difficult to study the pharmacokinetics of magnesium compounds in humans. Modeling of deep magnesium deficiency, studying the level of magnesium in bones and other tissues, which have proven themselves well in experiments, are not applicable here. It must be remembered that the organization of objective studies of the pharmacokinetic parameters of magnesium compounds in humans should take into account the need to control the intake of magnesium from food, natural circadian (daily) changes in the level of endogenous magnesium in the blood, and determine the capacity of magnesium depots.
Chemical properties
Magnesium hydroxide decomposes when heated above 350 ° C in vacuum and at 800 ° C in air:
The compound is a weak base, interacts with acids, ammonium salts and acid oxides (actively absorbs carbon dioxide from the air):
When heated, it reacts with certain nonmetals, which result in the formation of the corresponding hydrides:
Complex formation with inorganic ligands for Mg 2+ cations is uncharacteristic (unstable complexes with oxygen molecules are known for magnesium halides), therefore Mg (OH) 2 is insoluble in meadows.
Magnesium Hydroxide
Magnesium hydroxide
Chemical properties
Inorganic compound, basic metal hydroxide Mg. Under standard conditions, it is an amorphous substance, practically insoluble in water, soluble in ammonium salts. Chemical formula of Magnesium Hydroxide: Mg(OH)2. It exists in nature as the mineral brucite. Molecular weight = 58.3 grams per mole.
Chemical properties of Magnesium Hydroxide. A weak base does not dissolve in water, but even a small amount of dissolved compound gives the solution an alkaline reaction. A characteristic coloring of the indicators is observed.
The product is quite unstable to high temperatures and decomposes at 350 degrees Celsius.
Reacts with acids, acid oxides (forms salt and water); with concentrated alkali ( hydroxymagnesates ).
The substance is obtained using reactions of soluble Mg salts and alkali, a solution of Mg chloride with calcined dolomite , and metallic Mg with water vapor. As a result, a white amorphous, cheesy precipitate always falls out; the color of the precipitate is white or yellowish due to impurities in the reagents.
Mg hydroxide is used:
- for wastewater treatment as a flocculant;
- in the production of thermoplastic polymers;
- as a reagent for binding sulfur dioxide to produce magnesium oxide ;
- as part of detergents and cleaning products;
- in the production of toothpaste and refined sugar;
- in the form of a food additive under code E528 ;
- in medicine to neutralize stomach acids and as a laxative.
pharmachologic effect
Antacid, laxative.
Pharmacodynamics and pharmacokinetics
Magnesium hydroxide has the ability to neutralize free hydrochloric acid contained in gastric juice.
Application
Magnesium hydroxide is used as an intermediate in the synthesis of magnesium metal. It is used to purify sugar, water in boiler rooms, and in the production of toothpastes.
In medicine
Magnesium hydroxide is widely used as an antacid for high acidity of gastric juice (gastritis, gastric and duodenal ulcers). It is part of the drug “Maalox” (an acronym for “ma navoz al Yuminov oxid ”), as well as its analogue “almagel”, which reduce acidity.
Neutralizing the perchloric acid contained in the stomach turns into magnesium chloride, which has a laxative effect. Used for poisoning with acids and arsenic compounds.
NikoMag
Highly effective non-toxic inorganic fire retardant.
It is the optimal choice for the production of compounds based on PA, PP, PE, EVA ● used in the pharmaceutical industry (laxatives, antacids and other magnesium-containing medications) ● used in the food industry as a food additive E-528 (acidity regulator, color stabilizer, etc.) .d.
) ● in the production of additives for lubricating oils ● in the production of magnesium-containing compounds ● in the production of catalysts ● in the production of pigments ● in the production of cosmetics and personal care products.
Quality parameters
Uncoated magnesium hydroxide (A5, A7, A10) >> Fatty acid-coated magnesium hydroxide (M5F, M7F, M10F) >> Silane-coated magnesium hydroxide (M5S, M7S, M10S) >>
Uncoated magnesium hydroxide:
| 1 Appearance |
| 2 Mass fraction of magnesium hydroxide, %, not less |
| 3 Mass fraction of volatile substances at 105 °C,%, no more |
| 4 Mass fraction of iron (Fe), ppm, no more |
| 5 Mass fraction of calcium (Ca), ppm, no more |
| 6 Mass fraction of chlorides (Cl-), ppm, no more |
| 7 Mass fraction of sulfur (S), ppm, no more |
| 8 Mass fraction of sodium (Na), ppm, no more |
| 9 Bulk density, g/cm3, not less |
| 10 Specific surface area, m2/g |
| 11 Whiteness, %, not less |
| Residue when sifted on a 45 µm sieve, %, no more (determined by laser diffraction) |
| 13 Particle size distribution, microns: diameter of 10% of particles (d10) no more than diameter of 50% of particles (d50) no more than diameter of 90% of particles (d90) no more |
| 14 Surface treatment |
| 15 Crystal shape |
Magnesium hydroxide coated with fatty acids:
| 1 Appearance | |
| 2 Mass fraction of magnesium hydroxide, %, not less | |
| 3 Mass fraction of volatiles at 105 °C,%, no more | |
| 4 Mass fraction of iron (Fe), ppm, no more | |
| 5 Mass fraction of calcium (Ca), ppm, no more | |
| 6 Mass fraction of chlorides (Cl-), ppm, no more | |
| 7 Mass fraction of sulfur (S), ppm, no more | |
| 8 Mass fraction of sodium (Na), ppm, no more | |
| 9 Bulk density, g/cm3, not less | |
| 10 Specific surface area, m2/g | |
| 11 Whiteness, %, not less | |
| 12 Residue when sifted on a 45 µm sieve, %, no more (determined by laser diffraction) | |
| 13 Particle size distribution, microns: diameter of 10% of particles (d10) no more than diameter of 50% of particles (d50) no more than diameter of 90% of particles (d90) no more | |
| 14 Surface treatment | Fatty acid coated |
| 15 Crystal shape |
*The standard is given for an uncoated product
Magnesium hydroxide coated with silanes:
| 1 Appearance |
| 2 Mass fraction of magnesium hydroxide, %, not less |
| 3 Mass fraction of volatiles at 105 °C, %, no more |
| 4 Mass fraction of iron (Fe), ppm, no more |
| 5 Mass fraction of calcium (Ca), ppm, no more |
| 6 Mass fraction of chlorides (Cl-), ppm, no more |
| 7 Mass fraction of sulfur (S), ppm, no more |
| 8 Mass fraction of sodium (Na), ppm, no more |
| 9 Bulk density, g/cm3, not less |
| 10 Specific surface area, m2/g |
| 11 Whiteness, %, not less |
| 12 Residue when sifted on a 45 µm sieve, %, no more (determined by laser diffraction) |
| 13 Particle size distribution, microns: diameter of 10% of particles (d10) no more than diameter of 50% of particles (d50) no more than diameter of 90% of particles (d90) no more |
| 14 Surface treatment |
| 15 Crystal shape |
*The standard is given for an uncoated product
An individual approach to the client is the basis of the production process. The product is optionally modified with any type of sizing material (stearic acid, amino and vinyl silanes). The particle size distribution and specific surface area are adjusted accordingly.
PACKAGE
Synthetic magnesium hydroxide is shipped in three-layer bags with a net weight of 20 kg or small bags with a net weight of 500 kg by road and rail, including container shipments.
CERTIFICATION
ISO 9001; ISO 2200:2005; HACCP Codex Alimentarius;; Halal certificate; Kosher Certificate; REACH 01-2119488756-18-0034
APPLICATION
- Highly effective non-toxic inorganic fire retardant. An excellent choice for the production of compounds based on PA, PP, PE, EVA.
- In the pharmaceutical industry (laxatives, antacids and other magnesium-containing drugs)
- In the food industry as a food additive E-528 (acidity regulator, color stabilizer, etc.)
- In the production of lubricating oil additives
- In the production of magnesium-containing compounds
- In the production of catalysts
- As pigments
- In the production of cosmetics and personal care products.