Systemic autoimmune diseases are among the most severe chronic non-infectious human diseases. Lack of knowledge about the specific etiological factors of most rheumatic diseases makes it impossible to carry out effective etiotropic therapy. That is why their pharmacotherapy remains one of the most difficult problems of modern clinical medicine. Improving knowledge in the field of clinical immunology regarding the pathogenetic mechanisms of the development of rheumatic diseases, the development of the concept of “pathogenetic therapy”, together with advances in pharmacology, contribute to a significant improvement in the life prognosis of patients. The “pathogenetic” category includes a large number of drugs with different chemical structures and pharmacological properties. They are united by the ability, to a greater or lesser extent and through different mechanisms, to suppress inflammation and/or pathological activation of the immune system. Most of these drugs were developed for the treatment of cancer rather than rheumatic diseases or for the needs of transplantology [35].
Mycophenolate mofetil (MMF; CellCept; F. Hoffmann-La Roche Ltd., Switzerland) is a synthetic morpholinoethyl ester of mycophenolic acid (MPA) and is its precursor. MPA is a weak organic acid isolated as a product of natural fermentation of Penicillium stoloniferum in 1913. It is a non-competitive, reversible inhibitor of inosine monophosphate dehydrogenase (IMPDH), the enzyme responsible for the rate-limiting stage of de novo synthesis of guanosine nucleotides. Inhibition of IMPDH leads to a consistent decrease in the formation of xanthine monophosphate, guanosine monophosphate, guanosine triphosphate and deoxyguanosine triphosphate from inosine monophosphate, which are necessary for the synthesis of lymphocytic DNA, which leads to the interruption of lymphocyte replication in the S-phase. MPA has a higher affinity for type II IMPDH (it is this “inducible” isoform that predominates in proliferating lymphocytes) compared to type 1 IMPDH, which is a “constitutional” enzyme characteristic of non-dividing cells [1].
At very low (nanomolar) concentrations, MPA inhibits the proliferation of mitogen-stimulated human peripheral blood B and T lymphocytes in vitro. MPA also inhibits a mixed culture of lymphocytes, but has no effect on most dividing cells of other types [1]. To suppress the proliferation of mitogen-stimulated fibroblasts or endothelial cells, the concentration of MPA must be 10 times higher (1 μmol/L) than to suppress lymphocytes (100 nmol/L). Thus, the cytostatic effect of MPA and MMF is limited mainly to lymphocytes, which makes the drug relatively well tolerated [1]. Among other mechanisms of action of MPA, attention is drawn to the dose-dependent inhibition of the expression of markers of activation and proliferation of lymphocytes, as well as in vivo suppression of the formation of a population of cytotoxic lymphocytes capable of lysing allogeneic cells [1].
Depletion of guanosine nucleotide reserves under the influence of MPA negatively affects not only DNA synthesis, but also the process of glycosylation of adhesion molecules. MPA disrupts the process of transfer of mannose and fucose to glycoproteins in the composition of adhesion molecules, thus leading to difficulty in the interaction of endothelial cells and lymphocytes. Ultimately, disruption of the expression of adhesion molecules suppresses the entry of lymphocytes into areas of inflammation [2].
MPA reduces the formation of antibodies in cultures of human lymphocytes and spleen cells. In kidney transplant patients, MMF suppressed the humoral immune response to antithymocyte and antilymphocyte drugs, as well as to influenza vaccine antigens [3]. Such suppression of the humoral response is undoubtedly useful in the treatment of antibody-mediated diseases, incl. and rheumatic. In addition, MPA has the ability to inhibit the induced or so-called pathological, non-constitutional form of nitric oxide synthetase [4].
MPA was initially studied as an antitumor agent, mainly by Japanese researchers, and in the 70s. last century, the effectiveness of MPA for psoriasis was shown. But only in the late 80s. Allison and his group developed MMF as an antimetabolic immunosuppressant [5]. MMF was initially studied as a treatment and prevention of acute rejection of allogeneic transplants of various organs (kidney, liver, heart, pancreas) as part of combination therapy [1,6,7]. In large randomized controlled trials in patients undergoing kidney or heart transplantation, MMF reduced the incidence of rejection, demonstrating significantly higher efficacy than azathioprine [7,8]. It has been shown that MMF can stop the already begun process of acute rejection of heart, kidney and liver transplants [9]. The drug is also used to treat chronic vasopathy of heart and lung transplants [9]. In patients with chronic nephrotoxicity caused by cyclosporine A, additional administration of MMF led to an improvement in renal function [10]. It should be noted that the effectiveness of immunosuppression provided by MMF made it possible to reduce the use of glucocorticoids and cyclosporine A [9].
To date, there are a small number of observations regarding the use of MMF in autoimmune diseases - rheumatoid arthritis [11,12], systemic lupus erythematosus (SLE), systemic vasculitis [13,14], psoriasis, pemphigus [15], atopic eczema, autoimmune hemolytic anemia, inflammatory bowel diseases [16], autoimmune hepatitis, primary biliary cirrhosis, myasthenia gravis, dermatomyositis [17], scleroderma [18], glomerulonephritis [19].
According to experimental studies, the administration of MMF reduces the severity of proteinuria, glomerulosclerosis, interstitial infiltration by macrophages and T-lymphocytes in partially nephrectomized rats. At the same time, the antilymphocyte effect of MMF affects not only immunological, but also “non-immunological” mechanisms of progression of pathological changes in kidney tissue: inhibition of lymphocytes, severity of glomerulosclerosis and interstitial fibrosis, suppression of proliferation of renal tubular cells [20].
The use of a combination of MMF and low doses of glucocorticoids as maintenance therapy in patients with ANCA-associated vasculitis (Wegener's granulomatosis and microscopic polyangiitis) has brought encouraging results. After achieving remission on the background of cyclophosphamide and glucocorticoids, patients received 2 g of MMF per day for 15 months, and not only a low frequency of disease relapses was recorded (less than 10%), but also good tolerability and a steroid-sparing effect of MMF were noted [13].
A positive effect of MMF on skin manifestations of dermatomyositis, resistant to traditional therapy with glucocorticoids, aminoquinoline drugs and methotrexate, was noted. Within 6-20 months of using MMF, it was possible to achieve control over the activity of skin pathology and reduce the maintenance dose of glucocorticoids [17].
Currently, the effectiveness and tolerability of MMF in patients with SLE has been studied in a few open trials, including primarily patients with refractory lupus nephritis. All studies noted a positive effect of MMF, manifested by a decrease or stabilization of serum creatinine and urea, normalization of the level of complement C3 component and antibodies to double-stranded DNA [9,5,21]. Along with a decrease in the activity of the renal process, almost all researchers noted a positive effect of the drug on other manifestations of SLE (lesions of the skin and joints), a decrease in the activity of the disease in general [22,23].
Attempts to use MMF in children with lupus nephritis, in which glucocorticoids and cytotoxic therapy are almost always associated with the development of severe adverse reactions, deserve undoubted attention. Available reports indicate the effectiveness of MMF both in relation to the manifestations of nephritis, refractory to “traditional” therapy, and in relation to reducing the general and immunological activity of SLE, along with achieving a steroid-sparing effect with good tolerability of the drug [24,25].
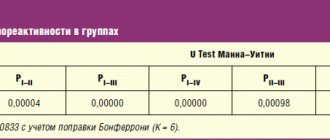
Of particular interest are the results of the only randomized controlled trial of MMF in SLE [26], in which the efficacy and tolerability of MMF and oral cyclophosphamide were assessed in 42 patients with diffuse proliferative lupus nephritis. In the compared groups, there were no significant differences in either the frequency of complete and partial remissions, or the frequency of exacerbations. Moreover, the frequency of infectious complications during the observation period was higher in the group of patients receiving cyclophosphamide compared to MMF. Complications such as amenorrhea, increased hair loss and leukopenia occurred only during treatment with cyclophosphamide and did not occur in patients receiving MMF. Notably, deaths were also reported only in the cyclophosphamide group [26].
All researchers who prescribed MMF are unanimous in their opinion that the drug has an acceptable range of side effects and is well tolerated. The main side effects of MMF are reactions from the gastrointestinal tract, such as diarrhea, nausea, vomiting, gastroenteritis [1,27]. Isolated cases of esophagitis, acute gastric and duodenal ulcers have also been described [27]. In second place in terms of frequency of occurrence are hematological disorders: leukopenia (in 19-35% of patients), anemia (in 25%) and thrombocytopenia (in 8-10%) [1,28]. It should be noted that when the dose of MMF is reduced, leukopenia is easily eliminated. Like any other immunosuppressant, MMF increases the susceptibility of patients to infection. The most common infections with MMF were cytomegalovirus infection and infections caused by the Herpes simplex and Herpes zoster viruses, but severe infectious complications were rare [1,27,28].
Assessing the tolerability profile of MMF is complicated by the high incidence of adverse events caused by the simultaneous administration of other immunosuppressants, so it is impossible to unequivocally regard all reported side effects as a result of the use of MMF.
Patients receiving immunosuppressive therapy have an increased risk of developing lymphomas and other malignancies, and the risk depends not so much on the use of any specific drug, but on the intensity and duration of immunosuppression [29]. In large clinical trials, the overall incidence of lymphoma or lymphoproliferative diseases in patients taking MMF was 1%[29]. In comparative studies, the incidence of malignant neoplasms with MMF was slightly higher than with azathioprine, but the small number of malignant neoplasms that developed during the observation period does not allow definite conclusions to be drawn [8]. In groups of patients with psoriasis and rheumatoid arthritis, long-term treated with MMF, no increase in the incidence of malignant tumors was recorded [30,31].
Preclinical studies of MMF in animals did not demonstrate any effect of the drug on fertility, but it caused a teratogenic effect in rats and rabbits. Despite the fact that to date, the birth of 5 healthy children from mothers on MMF therapy has been reported, effective contraception should be recommended during use and for 6 weeks after discontinuation of the drug [28].
As for other side effects, metabolic disorders such as hyperkalemia and hyperglycemia were observed more often with azathioprine than with MMF, and the development of allergic reactions with MMF was extremely rare [1]. In light of the possible use of MMF in patients with rheumatic diseases, primarily SLE, the absence of indications of nephrotoxicity of the drug is especially important [1].
To date, the economic aspects of the use of MMF as part of immunosuppression regimens have been studied only for kidney transplantation. Two US studies (cost-effectiveness model analysis and single-center effectiveness analysis) showed that MMF-containing regimens were associated with lower total costs in the first year after transplantation than azathioprine-containing regimens [32,33]. According to these analyses, the reduction in overall treatment costs of MMF compared with azathioprine was achieved primarily due to the significantly lower costs of treatment of rejection and associated hospitalization, which offset the high procurement cost of MMF. Another reason for the lower cost of MMF-containing regimens is the lower incidence of graft death and subsequent dialysis.
All of the above indicates that the use of MMF is a promising direction in the treatment of rheumatic diseases, especially SLE. In this regard, we carried out work to study the effectiveness and tolerability of MMF in 36 patients with SLE, in whom the most common manifestations of the disease were lesions of the central nervous system and kidneys, refractory to previous therapy with “traditional” immunosuppressants - glucocorticoids and cytotoxic drugs. Treatment with MMF was carried out for 6-12 months, the dose of the drug during the entire study period was 2 g per day [34].
During MMF therapy, the following results were obtained: improvement (clinically significant positive dynamics of symptoms and laboratory parameters) was observed in 48% of patients, stable condition (no negative dynamics) – in 38%, deterioration – in 14%. A significant decrease in disease activity noted in our patients was recorded already by the 3rd month of therapy.
The effect of MMF on the manifestations of SLE was different: the most sensitive to this drug were articular syndrome and headaches (the effect developed quite quickly in the vast majority of patients), there was a positive dynamics of cutaneous vasculitis, normalization of temperature, and improvement of intellectual and mnestic functions. One of the main distinguishing features that characterized patient “responders” to MMF therapy was a significantly lower level of peripheral blood lymphocytes at the end of the study. This fact may indicate a more pronounced antiproliferative effect of the drug against lymphocytes in this category of patients, which led to a positive effect on the manifestations of SLE.
Particularly noteworthy are the results regarding the significant positive dynamics of blood cells (especially platelets) during MMF therapy. The occurrence of cytopenias is one of the main adverse reactions of MMF, however, directly opposite results were obtained in our patients. The increase in the level of hemoglobin, leukocytes and platelets may have been due to a decrease in the synthesis of antibodies to blood cells and the number of T-lymphocytes producing myelosuppressive substances, as part of a decrease in the overall activity of SLE.
The effect of MMF on lupus nephritis has been controversial. In 40% of patients with nephritis, an antiproteinuric effect was obtained, in the same number there was no clinically significant dynamics of proteinuria, and in 20% there was an increase in protein loss in the urine. However, by the end of 6 months of MMF therapy in patients with lupus nephritis, on average in the group, there was a significant increase in the level of total protein, albumin, and a decrease in both systolic and diastolic blood pressure. During the entire study period, good renal functional capacity was maintained: creatinine levels were stable, there was a tendency to a decrease in urea levels in the group as a whole and an increase in glomerular filtration. As can be seen from the presented results, in our study the antiproteinuric effect of MMF was inferior in severity to the positive effect on most other manifestations of nephritis. This may be due to the presence in most patients of long-term kidney damage with a predominance of so-called non-immune pathogenetic mechanisms of nephropathy development and the absence of an “application point” for the action of MMF (which has a selective antiproliferative effect against activated lymphocytes). Our data showed that MMF is more effective in patients with “active” nephritis (high levels of proteinuria, arterial hypertension), combined with extrarenal and immunological activity of SLE. In addition, the best effectiveness of MMF was observed in patients with a shorter duration of the disease, which is understandable, since it is in the early stages of the disease that the processes of active immune inflammation dominate, a number of manifestations of which (proliferation of T-lymphocytes, synthesis of antibodies and nitric oxide, interaction of activated lymphocytes and endothelial cells, etc.) MMF acts.
We, like other researchers, have noted the steroid-sparing effect of MMF. In most patients, especially when taking prednisolone in doses above 15 mg per day, it was possible to significantly and quickly reduce the dose of oral glucocorticoids. This allows us to discuss possible modifications of treatment regimens for SLE using MMF: firstly, to use suppressive doses of glucocorticoids for a shorter time when the disease is highly active, and secondly, to quickly switch to small maintenance doses of prednisolone, which will help reduce the frequency and severity of side effects reactions to steroid therapy.
MMF was well tolerated by patients in our study, despite the high (for autoimmune diseases) daily dose. Adverse reactions occurred in 36% of patients, but they were not severe and only in 4 cases required premature cessation of treatment, and in one of them - on its own. Moderately severe gastrointestinal disorders were most often recorded. No severe infectious complications were observed. On the contrary, while taking MMF, there was a significant decrease in the incidence of infectious diseases compared to the previous 6-month period, and in more than 1/3 of patients they were not recorded at all. This fact may indicate the selectivity of the immunosuppressive effect of MMF compared to “traditional” cytotoxic drugs that patients took before MMF was prescribed.
Reducing the incidence of severe infectious diseases with MMF use is important. Research in the field of SLE therapy is aimed at finding the most effective and safe drugs, and both qualities are of equal value. Both foreign and our own results are encouraging in terms of good tolerability of the drug. Efficacy against manifestations of SLE activity, along with the good tolerability of MMF (primarily, the minimal incidence of infections and cytopenias) may have undoubted practical value, since it allows the use of this drug in patients with unsatisfactory tolerability of other drugs (primarily cyclophosphamide).
In conclusion, it should be noted that the data available today allow us to discuss the use of MMF as an alternative to “traditional” cytotoxic drugs, especially when the latter are insufficiently effective or intolerable. However, to determine the specific place of MMF in the treatment of patients with SLE and other rheumatic diseases, long-term, controlled studies involving a large number of patients are necessary.
Mycophenolate mofeyil
Acyclovir.
With the simultaneous use of MMF and acyclovir, higher plasma concentrations of MMF and acyclovir were observed than when each drug was administered separately. Since plasma concentrations of MPAG, like acyclovir, are increased in renal failure, there is a possibility that the two drugs compete for tubular secretion, which could lead to further increases in the concentrations of both drugs.
Antacids and proton pump inhibitors (PPIs)
. When the drug Mycophenolate mofetil was used together with antacids (aluminum and magnesium hydroxide) and with proton pump inhibitors (lansoprazole and pantoprazole), a decrease in the concentration of MPA was observed. However, there was no significant difference between the rates of transplant rejection in patients taking Mycophenolate mofetil concomitantly with and without PPI drugs. This conclusion theoretically extends to antacids, since when they are taken simultaneously with the drug Mycophenolate mofetil, the concentration of MPA decreases to a much lesser extent than when taken simultaneously with the drug Mycophenolate mofetil with a PPI.
Cholestyramine.
After administering a single dose of MMF 1.5 g to healthy volunteers who had previously taken 4 g of cholestyramine 3 times a day for 4 days, a decrease in MPA AUC by 40% was observed. Caution must be exercised during the simultaneous use of MMF and drugs that affect enterohepatic recirculation (see section "Special Instructions").
Cyclosporine.
MMF does not affect the pharmacokinetics of cyclosporine. However, cyclosporine affects the enterohepatic recirculation of mycophenolic acid (IPA), which may result in an increase in AUCMPA of approximately 30% when cyclosporine is discontinued in renal transplant patients receiving mycophenolate mofetil and cyclosporine (compared with patients receiving sirolimus or belatacept with similar doses of the drug mycophenolate mofetil). On the contrary, when patients switch from cyclosporine therapy to therapy with immunosuppressants that do not affect the enterohepatic recirculation of MPA, a change in MPA exposure should be expected.
Telmisartan.
Simultaneous use with the drug mycophenolate mofetil leads to a decrease in the concentration of MPA by approximately 30%. Telmisartan affects the elimination of MPA by increasing the expression of peroxisome proliferator-activated receptor gamma, which in turn increases the expression and activity of the UGT1A19 gene. There were no clinical drug interactions observed when comparing graft failure rates and adverse event profiles in patients receiving Mycophenolate mofetil with or without concomitant telmisartan therapy.
Ganciclovir.
Based on the results of a study with a single oral dose of recommended doses of MMF and intravenous administration of ganciclovir, taking into account the known effect of renal impairment on the pharmacokinetics of MMF (see sections "Pharmacokinetics in special clinical situations" and "Special instructions") and ganciclovir, it can be assumed that the simultaneous use of these two drugs (competing in the process of tubular secretion) will lead to increased concentrations of MPAG and ganciclovir. A significant change in the pharmacokinetics of MPA is not expected, so there is no need to adjust the dose of MMF. If MMF and ganciclovir (or its prodrugs, such as valganciclovir) are prescribed to patients with renal insufficiency, patients should be carefully monitored.
Oral contraceptives.
MMF does not affect the pharmacokinetics of oral contraceptives. In a study involving 18 women with psoriasis, while taking the drug Mycophenolate Mofetil (1 g 2 times a day) for 3 menstrual cycles with combined oral contraceptives containing ethinyl estradiol (0.02-0.04 mg) and levonorgestrel (0.05 -0.2 mg), desogestrel (0.15 mg) or gestodene (0.05-0.1 mg), there was no clinically significant effect of Mycophenolate Mofetil on the concentrations of progesterone, luteinizing hormone (LH) and follicle-stimulating hormone (FSH). ). Thus, Mycophenolate Mofetil has no effect on the suppression of ovulation under the influence of oral contraceptives.
However, while taking Mycophenolate Mofetil, in addition to oral contraceptives, it is necessary to use other methods of contraception (see section “Pregnancy and lactation”).
Trimethoprim/sulfamethoxazole, norfloxacin, metronidazole.
They do not affect the systemic exposure of MPA when prescribed with one of the antibacterial drugs. But simultaneous use of the drug Mycophenolate Mofetil in combination with norfloxacin and metronidazole reduces the AUC0-48 MPA by 30% after a single dose of Mycophenolate Mofetil.
Tacrolimus.
With simultaneous use, there was no effect on the AUC and maximum concentration (Cmax) of MPA in patients after liver and kidney transplantation. In patients after kidney transplantation, the administration of Mycophenolate Mofetil did not affect the concentration of tacrolimus. In patients with a stable liver transplant, the AUC of tacrolimus after repeated doses of MMF at a dose of 1.5 g twice daily increased by approximately 20%.
Sirolimus.
In patients after kidney transplantation, simultaneous use of Mycophenolate Mofetil and cyclosporine led to a decrease in MPA exposure by 30-50% compared to patients receiving a combination of sirolimus and Mycophenolate Mofetil.
Rifampicin.
After dose adjustment, a decrease in MPA exposure was noted by 70% (AUC0-12). In patients after simultaneous heart and lung transplantation, monitoring of MPA exposure and dose adjustment of Mycophenolate Mofetil is recommended to maintain the clinical effect when administered together.
Ciprofloxacin and amoxicillin in combination with clavulanic acid.
In patients after kidney transplantation, in the days immediately after oral administration of ciprofloxacin or amoxicillin in combination with clavulanic acid, a decrease in the minimum concentration of MPA by 54% was observed. With continued antibiotic therapy, this effect decreases and disappears after cessation of therapy. The clinical significance of this phenomenon is unknown, since changes in trough concentrations may not adequately reflect changes in total MPA exposure.
Other interactions.
With simultaneous administration of probenecid and MMF to monkeys, a 3-fold increase in the AUC of MPCG in plasma was noted. Thus, other drugs undergoing tubular secretion may compete with MPAG, resulting in increased plasma concentrations of MPAG or another drug that is also undergoing tubular secretion.
Sevelamer.
Concomitant use of sevelamer and MPA in adults and children reduced Cmax and AUC0-12 of MPA by 30% and 25%, respectively. Sevelamer and other non-calcium containing phosphate binders should be administered 2 hours after taking Mycophenolate Mofetil to reduce the effect on the absorption of MPA.
Live attenuated vaccines.
Should not be administered to immunosuppressed patients. Antibody production in response to other vaccines may be reduced (see section "Special Instructions").
Modern view on the treatment of systemic lupus erythematosus
Ph.D. N.G. Klyukvina, S.V. Shekshina, corresponding member. RAMS, professor E.L. Nasonov
MMA named after I.M. Sechenov, Institute of Rheumatology RAMS, Moscow
Systemic lupus erythematosus (SLE) is an autoimmune rheumatic disease, the pathogenesis of which is based on defects in immunoregulation, leading to uncontrolled hyperproduction of autoantibodies to the components of one’s own tissues and the development of chronic inflammation affecting many organs and systems.
Intense interest in SLE over the past 50 years has improved diagnostic methods, but patient management continues to be challenging. The development of treatment methods is hampered primarily by the unknown etiology of the disease, the large variability of clinical manifestations, the possibility of both long-term spontaneous remissions and a malignant, rapidly progressing, sometimes fulminant course [1]. To control the disease, almost the entire arsenal of anti-inflammatory and cytotoxic drugs existing in medicine is currently used, the use of which has significantly improved the prognosis of patients’ lives. If before 1970 the life expectancy of only 40% of patients with SLE exceeded 5 years, then currently the 5-year survival rate is 90% or more [2].
In this regard, it is difficult to overestimate the importance of glucocorticoids (GC), the effect of which occurs almost immediately after administration. Long-term observations have shown that GCs have been and remain the drugs of choice in the acute course of the disease with visceral manifestations. However, already in the early stages it became clear that long-term glucocorticoid therapy in patients with SLE raises a number of questions regarding doses, duration of treatment and prevention of complications associated with taking potent drugs. Glucocorticoid therapy has been improved over the years: dosage forms have been modified, certain dosage provisions have been established in accordance with the degree of disease activity and certain visceral pathology. The view has become stronger that GCs should be given to SLE patients for many years, mostly for life, moving from high doses in the high activity phase to maintenance and maintaining this dose even during clinical remission.
A new stage in the use of GCs for SLE was the introduction of the method of intravenous administration of ultra-high doses of “pulse therapy,” which turned out to be very effective in previously incurable patients. Available data indicate a significant immunosuppressive effect of intravenously administered high doses of GC already on the first day. It is believed that loading doses of GC (primarily methylprednisolone) stop the formation of immune complexes, are deposited to a greater extent in inflamed tissues, and block the damaging effects of lymphotoxins. The anti-inflammatory and immunoregulatory effect of pulse therapy is largely due to the effect on the cytokine system, tumor necrosis factor and suppression of transcription of metalloproteinase and lipocortin genes.
Over the years of using pulse therapy, the methodology for its implementation has also changed. First, the concept of using this method only when other types of treatment does not help has been revised. A certain category of patients has been identified (young age, rapidly progressing lupusnephritis, high immunological activity) in whom this method should be used at the onset of the disease or immediately during any exacerbation.
Secondly, “classical” pulse therapy (daily for 3 consecutive days at the rate of 1520 mg per kg of patient weight) is not always enough. In order to increase effectiveness, in some cases loading doses of methylprednisolone are prescribed at intervals of several weeks over several months. To enhance the impact on immunopathological processes, the programmatic prescription of pulse therapy with methylprednisolone can be enhanced by the addition of cyclophosphamide, and in some cases, intravenous administration of methylprednisolone and cyclophosphamide is continued for 510 days to achieve a clinical effect. A treatment strategy is developed in a special way for patients with ineffectiveness of standard pulse therapy programs with methylprednisolone and cyclophosphamide, in cases of resistance to prescribed drugs, as well as in the presence of a combination of several prognostically unfavorable factors. In such situations, the most promising is synchronous intensive therapy, which is based on a combination of pulse therapy and extracorporeal treatment methods (plasmapheresis) [3].
GC therapy alone does not suppress activity in some forms of SLE. Since the 60s, cytostatic immunosuppressants, aminoquinoline derivatives and other drugs have been included in the treatment complex, which, along with GCs, have become a kind of basic therapy.
Most often, cyclophosphamide, azathioprine and chlorobutine are used for SLE; in recent years, methotrexate has been successfully prescribed for some forms. Indications for the inclusion of cytostatic immunosuppressants in the complex treatment of patients with SLE are currently considered to be active lupus nephritis and generalized vasculitis, high overall disease activity and resistance to GCs; the appearance of adverse reactions of these drugs already in the first stages of treatment, the need to reduce the maintenance dose of prednisolone. The introduction of cytostatics into the treatment complex made it possible to suppress the disease activity against the background of lower doses of GC and increase the survival rate of patients, primarily with lupusnephritis. With regular monitoring and individual selection of dose and drug, and careful monitoring of therapy, it was possible to significantly reduce the number of adverse reactions and complications.
Aminoquinoline derivatives have not lost their importance in patients with SLE without severe visceral manifestations and during the period of reducing doses of GCs and cytostatics to maintain remission. A detailed study of the mechanisms of action of these drugs, which revealed anti-inflammatory, antiplatelet, hypolipidemic, photoprotective, antioxidant, antimicrobial and analgesic effects, allowed us to take a fresh look at the prospects for their inclusion in the treatment regimen for SLE [4].
However, despite the progress achieved, the management of patients with SLE remains one of the most challenging problems in modern rheumatology. In terms of the combination of effectiveness and safety, drugs that affect immune inflammation, GC, cyclophosphamide, azathioprine, chlorbutin and others, do not always satisfy clinicians. In addition, in many patients, early administration of adequate doses of GCs and cytotoxic drugs does not avoid irreversible damage to vital organs and systems (primarily the kidneys and central nervous system), and is also often associated with the development of severe, potentially fatal adverse reactions (intercurrent infection , cytopenia, hemorrhagic cystitis, osteoporetic fractures, an increase in the number of malignant neoplasms, etc.). All this determines the need to study new approaches to pharmacotherapy for SLE. Improvement of methods of influencing the immune process occurs in two directions: changing traditional modes of their use and introducing new drugs into practice.
The application of new therapeutic techniques is the impact on lymphocytes (bone marrow transplantation, the use of nucleoside analogues and extracorporeal treatments), the prevention of the formation and deposition of immune complexes, and the modification of the immune response by inducing antigen-specific tolerance or interaction with the cytokine system.
When considering new approaches to treatment, it should be noted that human autoimmune diseases, having their own unique characteristics, generally resemble the immunopathological processes that form the basis of the transplantation immune response. Therefore, it is not surprising that many modern types of immunotherapy for diffuse connective tissue diseases were first successfully used in organ and tissue transplantation [5].
Cyclosporine A has been of particular interest in recent years, as it is considered one of the most effective drugs with selective immunosuppressive activity. It is increasingly used in clinical practice for the treatment of many immunoinflammatory diseases of internal organs, including SLE. The specific mechanisms that determine the effectiveness of cyclosporine A (CsA) in SLE are not completely clear. Obviously, in terms of the nature of its effect on the synthesis of cytokines, CsA is very close to glucocorticoids. It cannot be excluded that one of the important mechanisms of action of CsA in SLE is associated with inhibition of interferon synthesis. Of interest is the ability of CsA to suppress the expression of the CD40 ligand on the Tlymphocyte membrane. It is known that monoclonal antibodies to the CD40 ligand are very effective in slowing down disease progression in mouse models of lupus-like disease [6]. CsA probably has similar activity.
Currently, some experience has been accumulated in the use of CsA in SLE. Back in the early 1980s, several open-label, short-term trials of the effectiveness of CsA in SLE were conducted using high doses (more than 5 mg/kg/day) of the drug. In 1981, CsA was first prescribed to 5 patients with SLE at a dose of 10 mg/kg/day for 7 weeks. However, in all cases, treatment was discontinued due to the development of side effects (primarily nephrotoxic) and arterial hypertension. Thus, the effectiveness of CsA was significantly compromised by the development of a large number of complications, which was most likely due to the use of high doses of the drug.
In recent years, a series of long-term (more than 2 years) open clinical trials have been conducted, which assessed the effectiveness of low (less than 5 mg/kg/day) doses of CsA in SLE. Most reports on the use of CsA in patients with SLE concern the use of this drug for lupusnephritis, and a pronounced antiproteinuric effect occurring during the first 23 months of therapy was observed in a significant number of patients [7]. A number of researchers have also shown the effectiveness of low doses of the drug for thrombocytopenia, anemia and leukopenia, skin manifestations of SLE, polyserositis and arthritis refractory to therapy. It should be noted that in the presence of a good effect of therapy, the side effects that developed in some patients were not severe and rarely served as a basis for interrupting treatment. Almost all researchers recorded the steroid-sparing effect of the drug.
The undoubted advantage of CsA compared to other drugs used to treat SLE is the lower incidence of both immediate and long-term side effects, primarily infectious complications and malignant neoplasms. For example, the risk of developing lymphoproliferative tumors during long-term treatment with CsA is very low - 0.050.14%, and discontinuation of the drug can lead to tumor relapse. Unlike other cytotoxic drugs, CsA has minimal teratogenicity [8].
Our own experience of prescribing CsA in patients with SLE confirms the results of other studies: when patients took low doses of the drug (on average 22.5 mg/kg/day), a decrease in disease activity, positive dynamics of clinical manifestations of SLE, primarily a decrease in daily proteinuria, were recorded. normalization of temperature, relief of arthralgia, reduction of the brightness of skin rashes. We believe that treatment with CsA has a positive effect on disease activity, affecting severe organ pathology, and the use of low doses and careful monitoring of therapy avoids the development of severe side effects. CsA can be considered an alternative second-line drug in cases of intolerance and ineffectiveness of glucocorticoids and cytostatics. In addition, the undoubted positive aspects of the inclusion of CsA in the treatment regimen for SLE should be considered a lower incidence of concomitant infection and the possibility of administration during pregnancy. There is preliminary evidence of a decrease in the level of anticardiolipin and antiplatelet antibodies during CsA therapy, as well as a preventive effect against the early development of atherosclerosis, which is of great importance for patients with SLE [9].
Encouraging results were also obtained when using another selective immunosuppressant, mycophenolate mofetil, in patients with SLE. Mycophenolate mofetil (Cellcept) is a synthetic morpholinoethyl ester of mycophenolic acid and is its precursor. After oral administration of mycophenolate mofetil, hepatic esterases completely convert it into the active compound mycophenolic acid, which is a non-competitive inhibitor of inosine monophosphate dehydrogenase, the rate-limiting enzyme for the synthesis of guanosine nucleotides. Since the functional activity of lymphocytes, to a greater extent than other rapidly dividing cells, depends on the synthesis of purines, the drug gives a more pronounced antiproliferative effect on lymphocytes and exhibits cytostatic rather than cytotoxic activity. In nanomolar concentrations, mycophenolic acid suppresses the proliferation of stimulated T and B lymphocytes of human peripheral blood in vitro, has an antiproliferative effect against mesangial cells of human and animal kidneys, and suppresses the formation of antibodies in cultures of human lymphocytes and spleen cells. In addition, depletion of gaunosine nucleotides under the influence of mycophenolic acid negatively affects not only DNA synthesis, but also the glycosylation of adhesion molecules. This suppression of the humoral response may be useful in the treatment of antibody-mediated diseases [10]. As an antimetabolic immunosuppressant, mycophenolate mofetil was initially studied for the treatment and prevention of acute rejection of allogeneic solid organ transplants. As a rule, this drug is used as part of combination therapy after transplantation, prescribing it instead of azathioprine, in combination with glucocorticoids and cyclosporine. In large randomized controlled trials in patients undergoing kidney or heart transplantation, mycophenolate mofetil demonstrated significantly higher efficacy than azathioprine in reducing the incidence of rejection.
Mycophenolate mofetil: general characteristics
1 Developed to suppress graft rejection
2 "Pro-medicine"
3 Active metabolite - mycophenolic acid
4 Non-competitive reversible inhibitor of inosine monophosphate dehydrogenase (IMDHP) type II
Mycophenolate mofetil for SLE: rationale for use
- Reduction in the severity of kidney damage in rats with partial nephrectomy
- Reduced rate of progression of kidney damage in NZBxNZW F1 and MRL/lpr mice
Mycophenolate mofetil for SLE: clinical application
1 Diffuse proliferative lupus nephritis, refractory to cyclophosphamide
2 Open-label (67 patients) and one randomized controlled trial
3 Reduction or stabilization of serum creatinine and proteinuria
4 Reducing activity (SLAM)
5 Reducing the dose of prednisolone
To date, data have been published in the literature regarding the use of mycophenolate mofetil in about 100 patients with refractory lupus nephritis. Therapy with mycophenolate mofetil in doses of 1.5–2 g/day led to a decrease in proteinuria, stabilization of serum creatinine levels, normalization of levels of the C3 component of complement and antibodies to DNA, and a decrease in SLE activity indicators [11]. In 2000, a group of researchers from Hong Kong published data concerning a comparative analysis of the effectiveness of two drug regimens - GC in combination with mycophenolate mofetil and GC in combination with traditional cytostatics in SLE patients with diffuse proliferative lupus nephritis. As it turned out, the effectiveness of the two different treatment regimens, assessed by a decrease in proteinuria, creatinine and increase in albumin, was identical in both groups after 12 months of therapy. At the same time, the frequency of concomitant infectious complications that developed was 2 times higher in the group receiving cyclophosphamide and azathioprine, and side effects such as amenorrhea, hair loss, and leukopenia were not recorded at all in patients taking mycophenolate mofetil [12]. Literary data, as well as our own experience in prescribing mycophenolate mofetil to patients with SLE, suggest that in patients with kidney damage, the drug may be a worthy therapeutic alternative to cyclophosphamide and azathioprine, with better tolerability.
Another direction in the treatment of SLE in recent years has been the use of certain immunomodulators, such as thalidomide, bindarit, nucleoside analogues (fludarabine, mizoribine, leflunomide). The use of these drugs in experimental models of lupus-like disease led to a decrease in proteinuria and increased survival of mice. Currently, some experience has been accumulated in the use of these drugs in patients with SLE [13]. Clinical trials of thalidomide were mainly conducted in patients with severe skin lesions resistant to antimalarial drugs and GCs. In the vast majority of patients, it was possible to achieve a good effect and reduce the dose of GC, while discontinuation of the drug did not lead to an exacerbation of symptoms. The main limitation with the use of thalidomide is its teratogenicity. In addition, the development of irreversible peripheral neuropathy, depending on the dose and duration of treatment, has been described [14].
There are separate reports on the use of lobenzarite in SLE, which has pronounced immunomodulatory activity and can suppress the synthesis of antibodies to DNA and inhibit the synthesis of IgM rheumatoid factor [15].
The results of an in vitro study indicate a synergistic effect of the combination of nucleoside analogues and cyclophosphamide; Similar treatment regimens have been successfully used for a long time in oncology. As for patients with SLE, there are isolated reports of the effectiveness of these drugs in patients with lupus nephritis; their steroid-sparing effect has been proven. At the same time, one cannot fail to note the high incidence of concomitant infectious complications, which raises the question of the safety of the use of these drugs and the risk/benefit ratio in patients with SLE [16].
The prospects for treating patients with SLE undoubtedly lie in biological methods of influence, using so-called biological agents. These drugs are developed to influence specific immunological processes, which include T cell activation, T cell interaction, production of antibodies to double-stranded DNA, activation of cytokines, and others. In this regard, the use of anti-idiotypic monoclonal antibodies and intravenous immunoglobulin offers great potential. There are limited data on the effectiveness of recombinant DNase, a DNA-cleaving enzyme, in experimental models of lupus. Administration of the drug to NZB/W mice with an active renal process led to a decrease in proteinuria and serum creatinine, but use in several patients with SLE has not yet given convincing positive results, despite the good tolerability of the drug [17]. The detection of elevated serum levels of IL10 in SLE patients and relatives, as well as their correlation with disease activity, provided the basis for the use of monoclonal antibodies to IL10. Preliminary results from several studies indicate a positive effect of antibodies against skin lesions, kidney lesions, arthritis and serositis refractory to glucocorticoid therapy [18].
Thus, the use of “biological” agents will be an undoubted prospect for the treatment of patients with SLE, especially since most of them do not have a generalized immunosuppressive effect.
Currently, autologous stem cell transplantation (ASCT) should be recognized as the most aggressive treatment method for SLE. By 2000, experience had been accumulated in the use of ASCT in slightly more than 30 patients with SLE [19]. Preliminary positive results undoubtedly require further confirmation. Long-term observation of patients is necessary, keeping in mind the possibility of inducing the development of malignant tumors. Despite the impression that this type of therapy is effective in cases of refractory and severe SLE, due to the accompanying high mortality rate, ASCT can be recommended only in the most severe, hopeless cases.
Attempts to treat SLE by modulating sex hormones, the imbalance of which is unconditionally recognized as a pathogenetic factor of the disease, have not lost their relevance. New drugs currently used include dehydroepiandrosterone and other androgens, estrogen antagonists (including tamoxifen and selective estrogen receptor modulators), and the prolactin inhibitor bromocriptine.
It has been shown in experimental models that administration of estrogen or male sex hormone antagonists can reduce disease activity. The first attempts to prescribe hormonal drugs concerned the synthetic androgen, 19nortestosterone, and gave conflicting results: clinical improvement in women was followed by a relapse of symptoms after discontinuation of the drug, while in men, negative dynamics were observed during treatment. It has been suggested that the lack of effect in males can be explained by the weak effect of 19nortestosterone, which does not affect endogenous testosterone production. Studying the effectiveness of dehydroepiandrosterone, a natural androgen with a moderate effect, made it possible to discuss the advisability of its use in mild forms of SLE. One placebo-controlled study showed the drug was twice as effective as placebo and was generally well tolerated. The effectiveness of dehydroepiandrosterone is primarily attributed to changes in adrenal sex hormone levels, primarily increased testosterone concentrations, although indirect release of mineralocorticoid and glucocorticoid hormones may also be important [20].
The use of oral contraceptives and estrogen replacement therapy has long been controversial in patients with SLE. However, recently, the effectiveness of selective estrogen receptor modulators has been demonstrated in experimental models, which has allowed us to take a new look at the prospects for their use in humans. It must be borne in mind that such therapy should be carried out with caution due to the potential risk of thrombotic complications, especially in patients with secondary antiphospholipid syndrome [21].
A series of studies are assessing the therapeutic activity of tamoxifen, a synthetic non-steroidal anti-estrogen that specifically binds to estrogen receptors, which is used to treat breast cancer in women. According to early clinical studies performed on small clinical material, tamoxifen did not have a significant effect on the course of the disease in women with SLE [22]. However, tamoxifen has recently been shown to slow the progression of the disease process in mice with experimental lupus-like disease induced by immunization with anti-DNA monoclonal antibodies. It is assumed that the beneficial effect of the drug on the course of SLE may be associated with a change in the synthesis profile of Th1 and Th2 cytokines, an increase in cortisol production and a decrease in prolactin levels [23, 24].
The association of hyperprolactinemia with SLE activity has been convincingly proven [25]. Administration of bromocriptine, a dopamine receptor agonist, leads to a decrease in prolactin levels. A randomized, placebo-controlled study in 66 patients with SLE, even in the absence of high prolactin levels, revealed a statistically significant decrease in prolactin levels compared to controls, accompanied by a decrease in disease activity [26].
Thus, preliminary results from tests in animal models or pilot studies in humans suggest the effectiveness of a number of pharmacological agents in SLE, which include both “nonspecific” immunoregulators and drugs that affect the profile of sex hormones.
One more aspect of the treatment of SLE should be mentioned. Despite the undesirability of polypharmacy in SLE, accumulated experience indicates the need for the use of a number of auxiliary drugs. This applies to the use of drugs that improve cerebral circulation and metabolism of brain cells (vinpocetine, pentoxifylline, Cerebrolysin, piracetam, etc.), antiplatelet agents, anticonvulsants, tranquilizers.
The presence of secondary antiphospholipid syndrome (APS) in SLE patients also requires adjustments to treatment regimens. A difficult problem is the prevention of recurrent thrombosis in APS. This is due to the heterogeneity of the pathogenetic mechanisms underlying APS, the polymorphism of clinical manifestations, and the lack of reliable clinical and laboratory indicators to predict the recurrence of thrombotic disorders. Patients with APS are prescribed indirect anticoagulants and antiplatelet agents (low doses of acetylsalicylic acid), which are widely used to prevent thrombosis. However, the use of high doses of indirect anticoagulants is associated with an increased risk of bleeding, so such therapy requires careful monitoring. Patients with APS often experience moderate thrombocytopenia, which is usually corrected with small doses of glucocorticoids. Sometimes, for GC-resistant forms of thrombocytopenia, low doses of acetylsalicylic acid, danazol, and warfarin are effective. Great hopes are placed on the use of low molecular weight heparin, as well as on the introduction of new methods of anticoagulant therapy based on the use of arginals, hyuidins, anticoagulant peptides and antiplatelet agents (monoclonal antibodies to platelets) [27].
An important area of pharmacotherapy for SLE is the prevention of the development or treatment of concomitant (often drug-induced) pathology, primarily “early” atherosclerosis, osteoporosis, and infectious complications, which have no less negative impact on life prognosis than the disease itself. This determines the need for a wider introduction of modern antihypertensive, hypolipidemic, antiosteoporetic and antimicrobial drugs. Since some of them, such as statins, antibiotics and possibly bisphosphonates, have anti-inflammatory and immunomodulatory activities, their use has the potential to improve the effectiveness of the treatment of inflammatory rheumatic diseases.
The question of dietary regimen for SLE has been raised again, since there is evidence of the influence of certain nutrients on the mechanism of inflammation development. A reduced content of linoleic acid in food leads to a decrease in the synthesis of prostaglandins and leukotrienes, which have a pro-inflammatory effect. With an increase in the content of unsaturated fatty acids in food, the intensity of the processes of inflammation and fibrosis formation decreases [1]. In this regard, it seems appropriate to study the effect of diets with a certain content of fatty acids on various manifestations of the disease, which will allow us to evaluate the effect of dietary regimens on the development of the pathological process.
Thus, today it is possible to quite effectively influence the pathological process in SLE. With the skillful use of potent drugs, it is possible not only to significantly improve the prognosis of patients with SLE, but also to avoid serious complications of the therapy. Despite the fact that the presented material cannot fully cover the diversity of approaches to the treatment of SLE, in general it still allows us to trace the main modern trends, primarily concerning drugs that have a high specificity in influencing the mechanisms of disease development and are characterized by fairly high efficiency and safety . At the same time, we must not forget about the development of new treatment methods that are not symptomatic, but pathogenetically targeted.
Literature:
1. Ivanova M.M. Systemic lupus erythematosus. Diagnosis and treatment. Wedge. Rheumatology, 1995, 1, 220.
2. Gladman DD, Urowitz MB Duboiss Lupus erythematosus. 5th Ed. Eds DJWaalace, BH Hahn, Baltimore, 1997, 12131228.
3. Solovyov S.K., Ivanova M.M., Nasonov E.L. Intensive therapy of rheumatic diseases. Publishing house ォMIKサ, Moscow, 2001.
4. Nasonov E.L. Anti-inflammatory therapy of rheumatic diseases. Moscow, publishing house ォMSITYサ, 1996, 169 181.
5. Nasonov E.L., Shtutman V.Z., Nasonova V.A. Prospects for the use of cyclosporine A in rheumatic diseases. Wedge. Medicine, 1994, 5, 1219.
6. Blank M., BenBassat M., Shoenfeld Y. The effect of cyclosporin A on early and late stages of experimental lupus. Arthritis and Rheumatism, 1992, 35, 11, 13501354.
7. Caccavo D., Lagana B., Mitterhofer A. et al. Longterm treatment of systemic lupus erythematosus with cyclosporine A. Arthritis and Rheumatism, 1997, 40 (1), 2735.
8. Cyclosporine. Clinical application in autoimmune diseases. Edited by David E. Yocum. Mosby Wolfe, 2000.
9. Walter D.H., Haendeler J., Galle J. et al. Cyclosporine A inhibits apoptosis of human endothelial cells by preventing release of cytochrome C from mitochondria. Circulation, 1998, 98, 11531157.
10. Kingdon EJ, McLean AG, Psimenou E. et al. The safety and efficacy of MMF in lupus nephritis: a pilot study. Lupus, 2001, 10, 60611.
11. Adu D., Cross J., Jayne DRW. Treatment of systemic lupus erythematosus with mycophenolate mofetil. Lupus, 2001, 10, 203208.
12. Chan TM, Li FK, Tang CSO et al. Efficacy of mycophenolate mofetil in patients with diffuse proliferative lupus nephritis. The New England Journal of Medicine, 2000, 343(16), 11561162.
13. Illei GG, Klippel JH Novel approaches in the treatment of lupus nephritis. Lupus, 1998, 7, 644648.
14. Stevens RJ, Andujar C, Edwards CJ et al. Thalidomide in the treatment of cutaneous manifestations of lupus erythematosus experience in sixteen consecutive patients. Br. J. Rheumat., 1997, 36, 353359.
15. Hirohata S., Ohnishi K., Sagawa A. Treatment of systemic lupus erythematosus with lobenzarit: an open clinical trial. Clin. And Exp. Rheumatol., 1994, 12, 261265.
16. Strand V. Biologic agents and innovative interventional approaches in the management of systemic lupus erythematosus. Current Opinion in Rheumatology, 1999, 11, 330340.
17. Davis JC, Manzi S, Yarboro C et al. Recombinant human Dnase in patients with lupus nephritis. Lupus, 1999, 8, 6876.
18. Llorente L., GarciaPadilla C., RichaudPatin Y. et al. Treatment of systemic lupus erythematosus with an antiinterluken10 monoclonal antibody. Arthrit. Rheum., 1998 (suppl.), 41, S109.
19. Tyndall A., Passweg J., Gratwohl A. Haemopoietic stem cell transplantation in the treatment of severe autoimmune diseases 2000. Ann.Rheum.Dis., 2001, 60, 702707.
20. Vollenhoven R, Engleman E, McGuire J. Dehydroepiandrosterone in systemic lupus erythematosus. Arthr. Rheum., 1995, 38 (12), 18261831.
21. Mok C, Lau CS, Ho CTK. Safety of hormonal replacement therapy in postmenopausal patients with systemic lupus erythematosus. Scand J Rheumat, 1998, 27, 342346.
22. Sturgess AD, Evans DT, Mackay IR, Riglar A. Effects of the estrogen antagonist tamoxifen on disease indices in systemic lupus erythematosus. J. Clin. Lab. Immunol., 1984, 13, 1114.
23. Levin J, Markhan MJ, Greenwald ES et al. Effects of tamoxifen treatment on cortisol metabolism and the course of the disease in advanced breast cancer. Cancer, 1981, 47, 13941397.
24. Liberman ME, Jordan VC, Fritsch M. Direct and reversible inhibition of estradiol stimulated prolactin synthesis by antiestrogen in vitro. J. Biol. Chem., 1983, 258, 47344740.
25. Walker SE, Allen SH, Hoffman RW Prolactin is a stimulator of disease activity in systemic lupus erythematosus. Lupus, 1995, 4, 39.
26. AlvarezNemegyei J., CovarrubiasCobos A., EscalanteTriay F. et al. Bromocriptine in systemic lupus erythematosus: a double blind, randomized placebo controlled study. Lupus, 1998, 7, 414419.
27. Nasonov E.L., Baranov A.A., Shilkina N.P. Vasculitis and vasculopathy. Yaroslavl, ォUpper Volgaサ, 1999, 540574.
Published with permission from the administration of the Russian Medical Journal