What are antibiotics?
Antibiotics are substances that can inhibit the growth of microorganisms or destroy them. According to the GOST definition, antibiotics include substances of plant, animal or microbial origin. Currently, this definition is somewhat outdated, since a huge number of synthetic drugs have been created, but natural antibiotics served as the prototype for their creation.
Classification of antibiotics:
- Antibacterial antibiotics inhibit the development of bacteria. Some of them, for example, benzyl penicillin, Macrolides, ristomycin (ristocetin, spontin), novobiocin and others, are active mainly only against gram-positive microbes, others, such as polymyxin, suppress the development of mainly gram-negative bacteria, others, for example, tetracyclines, levomycetin (chloramphenicol, chloromycetin), aminoglucosides (streptomycin, monomycin, kanamycin, neomycin and gentamicin), so-called broad-spectrum antibiotics, inhibit the growth of both many gram-positive and gram-negative bacteria.
- Antifungal antibiotics have a specific inhibitory effect on fungal growth. The antibiotics nystatin and levorin, used to treat candidiasis and other diseases caused by yeast-like fungi, have found widespread use in medical practice. The antibiotic amphotericin B is used to treat generalized and deep mycoses.
- Antitumor antibiotics. It has been established that some antibiotics inhibit the development of not only bacteria and fungi, but can also inhibit the proliferation of malignant tumor cells. Some of these drugs have found use in medical practice.
Antibiotics, or, as they are also called, antimicrobials, suppress pathogenic microorganisms - bacteria or fungi. But viruses are not organisms; they live inside human cells.
Amoxiclav in the treatment of bronchopulmonary infections
About the article
62859
0
Regular issues of "RMZh" No. 5 dated March 16, 2005 p. 264
Category: General articles
Authors: Lenkova N.I. 1, Evdokimova S.A. , Demchenkova E.Yu. 1 Federal State Autonomous Educational Institution of Higher Education “First Moscow State Medical University named after. THEM. Sechenov" of the Ministry of Health of Russia (Sechenov University)
For quotation:
Lenkova N.I., Evdokimova S.A., Demchenkova E.Yu. Amoxiclav in the treatment of bronchopulmonary infections. RMJ. 2005;5:264.
Bacterial infections of the respiratory system are one of the serious medical and social problems. The main direction in the treatment of infections of the upper and lower respiratory tract is the use of antibacterial drugs, leading to the suppression of the vital activity of microorganisms as a result of inhibition of a metabolic process specific to them (binding of an antibiotic with an enzyme or structural molecule of bacteria) [11].
Despite the availability of a large number of modern antibiotics, every attending physician always faces the problem of choosing the optimal drug. When choosing an antibacterial drug for the treatment of pneumonia and exacerbations of chronic bronchitis, it is necessary to take into account the age, severity of the patient’s condition, the presence of concomitant diseases, and conditions for the development of the disease. One of the groups of antibacterial drugs that have proven themselves for the treatment of infections of the respiratory system are semi-synthetic protected penicillins. Representatives of this group include Amoxiclav® (amoxicillin/clavulant, Lek, Slovenia), the high efficiency and safety of which has been proven by numerous studies. Amoxiclav is a broad-spectrum antibiotic, which is a combination of the semisynthetic penicillin amoxicillin and the b-lactamase inhibitor clavulanic acid. The ratio of the components of the drug for oral administration is 2:1, 4:1, 7:1, for the parenteral form – 5:1 [10]. Amoxiclav has high bactericidal activity, including against strains of microorganisms resistant to amoxicillin alone [6]. The activity of this drug is observed against [2,10]: • aerobic gram-positive bacteria (including strains producing b-lactamases): Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pyogenes, Streptococcus anthracis, Streptococcus pneumoniae, Streptococcus viridans, Enterococcus faecalis, Corynebacterium spp., Listeria monocytogenes; • anaerobic gram-positive bacteria: Clostridium spp., Peptococcus spp., Peptostreptococcus spp.; • aerobic gram-negative bacteria (including strains producing b-lactamases): Escherichia coli, Proteus mirabilis, Proteus vulgaris, Klebsiella spp., Salmonella spp., Shigella spp., Bordetella pertussis, Yersinia enterocolitica, Gardnerella vaginalis, Neisseria meningitidis, Neisseria gonorrhoeae, Moraxella catarrhalis, Haemophilus influenzae, Haemophilus ducreyi, Yersinia multocida (formerly Pasteurella), Campylobacter jejuni; * anaerobic gram-negative bacteria (including strains producing b-lactamases): Bacteroides spp., including Bacteroides fragilis. Clavulanic acid suppresses types II, III, IV and V b-lactamases, is inactive against type I b-lactamases produced by Enterobacter spp., Pseudomonas aeruginosa, Serratia spp., Acinetobacter spp. Clavulanic acid has a high affinity for penicillinases, due to which it forms a stable complex with the enzyme, which prevents the enzymatic degradation of amoxicillin under the influence of b-lactamases [2,4,9]. A wide spectrum of antimicrobial action and activity against amoxicillin-resistant strains make Amoxiclav indispensable in the treatment of bronchopulmonary infections, especially with a high risk of pathogens producing b-lactamases, mainly in patients with immunodeficiency, with nosocomial infections [1,5,8]. The pharmacological characteristics of amoxicillin and clavulanic acid are very similar. When administered intravenously, serum concentrations of both substances are many times higher than the required therapeutic concentrations. When taken orally, they are quickly absorbed into the blood. Peak serum levels of both compounds are achieved approximately one hour after dosing. Concomitant consumption of food does not affect absorption. The drug is well distributed in organs and tissues, creating sufficient concentrations to destroy strains of sensitive bacteria. In addition to blood plasma, high concentrations of Amoxiclav are observed in sputum, bronchial secretions, lung tissue, and pleural fluid. Amoxicillin/clavulanate is superior to ampicillin in terms of penetration into lung tissue [9]. Concentrations of amoxicillin in sputum are twice the concentrations of ampicillin when taking the same doses of the drug. Moreover, the concentrations of the first drug remain in the sputum at a therapeutic level for much longer. Both components of the drug are metabolized in the liver: amoxicillin - by 10% of the administered dose, clavulanic acid - by 50% [2,4,9]. The drug is excreted mainly by the kidneys (glomerular filtration and tubular secretion): 50–78% of the dose of amoxicillin and 25–40% of clavulanic acid are excreted unchanged within the first 6 hours after administration [2,4,9]. Side effects when using the drug are in most cases mild and transient. They are represented mainly by changes in the digestive tract and allergic reactions [2,4,9]. Amoxiclav is approved for use in all trimesters of pregnancy. The drug has several dosage forms: for oral administration: Amoxiclav in tablets in doses of 375 mg, 625 mg and 1000 mg, which allows its use in outpatient practice, and for parenteral administration - bottles of 600 mg and 1200 mg (Table 1). Amoxiclav can be combined with antibacterial drugs from other groups. The presence of various forms of Amoxiclav implies the possibility of both parenteral therapy and oral administration. In the treatment of mild (outpatient) forms of community-acquired pneumonia and exacerbations of chronic bronchitis, preference should be given to oral forms of the antibiotic. In severe cases of infection, the antibiotic must be administered parenterally. Step therapy is also highly effective, which involves switching from the parenteral route of administration of the drug to the oral route, provided that the patient’s condition is stabilized or the course of the disease improves [3]. This is usually done on the 2-3rd day from the start of treatment. Stepped antibacterial therapy can provide effective therapy for pneumonia and exacerbations of chronic bronchitis [3]. The average duration of parenteral antibiotic use is 2–3 days, and oral therapy is given for 5–7 days. We studied the effectiveness of Amoxiclav. The observation group consisted of 20 patients with radiologically confirmed pneumonia, the average age of the patients was 60.7 years. The condition of 6 patients was assessed as moderate, the rest as satisfactory. Treatment of all patients began with intravenous drip administration of the drug 1.2 g every 8 hours for 2–3 days. After clinical improvement was achieved, intravenous therapy was replaced by oral therapy. Amoxiclav was prescribed at a dose of 625 mg every 8 hours orally with food. The total duration of treatment with the drug averaged 9 days. The clinical effectiveness of Amoxiclav turned out to be high (100%), recovery was noted in all 20 patients observed. Bacteriological eradication was achieved in 16 patients (80%). The comparison group consisted of 20 patients with pneumonia who received cefotaxime according to the traditional parenteral regimen: 1 g intramuscularly every 8 hours, on average 8 days. Recovery in this group was observed in 80% of cases, in 10% of patients there was a decrease in infiltrative changes with complete relief of signs of bacterial infection. Bacteriological efficiency was 82.6%. Thus, the clinical effectiveness of Amoxiclav was higher, and the bacteriological effectiveness was comparable to the effectiveness of cefotaxime. The cost of a 7-day course of therapy with Amoxiclav according to a stepwise scheme is 42.51 USD. The cost of a 7-day course of cefotaxime therapy when administered intramuscularly (including consumables) is 49.77 USD. (with intravenous infusions, the cost increases by 1.3 times). The most important advantages of stepwise therapy compared to parenteral therapy include ease of use and improved economic indicators. They consist of reduced costs due to the lower cost of dosage forms of antibiotics for oral administration compared to parenteral ones, lower costs for parenteral antibiotics used in a short course, reduced costs for syringes, solutions for intravenous administration, reduced working hours of medical staff and reduced risk and number of post-injection complications. Stepped therapy is a cost-effective regimen that provides benefits for both the patient and the hospital. When used, the cost of treatment is reduced by 30–60% [7]. Severe pneumonia requires the use of parenteral drug administration, and in some cases, combination therapy using antibiotics of other groups. Literature 1. Avdeev S.N., Chuchalin A.G. "The role of bacterial infection and the choice of antibiotics in exacerbation of chronic bronchitis." // Consilium, No. 2, 2000 2. “Antibacterial drugs. Methods for standardization of drugs” edited by Khabriev R.U. // Medicine, 2004 3. Budanov S. V. “Stepped antibiotic therapy for infections.” // Clinical Bulletin, No. 4, 1996. 4. State Register of Medicines, 2004. 5. Ioffe L.Ts., Beisebaev N.A., Shatskikh V.V., Salimova S.S., Auelbekova G. A., Esetova G.U. "Amoxiclav in the treatment of lower respiratory tract infections." // 12 National Congress on Respiratory Diseases, 2002 6. Krivtsiov E.V., Prokhorovich E.A., Aleksanyan A.A., Makaryan A.S., Chibikova A.A. “Comparative characteristics of semisynthetic penicillins (ampicillin and amoxicillin/clavulanic acid) and fluoroquinolones (pefloxacin and ciprofloxacin) in the treatment of patients with community-acquired pneumonia.” // Medical file, No. 2, 1999 7. Nonikov V.E., Konstantinova T.D., Lenkova N.I., Argetkina I.N. "Pharmacoeconomic aspects of antibacterial therapy of pneumonia." // Infection and antimicrobial therapy, No. 2, 1999 8. Nonikov V. E., Konstantinova T. D., Lenkova N. I., Minaev V. I., Ritchik L. A. “The effectiveness of amoxicillin/potassium clavulanate in the treatment of bronchopulmonary infections in a hospital." // Antibiotics and chemotherapy, No. 10, 1997. 9. Vidal reference book, 2003. 10. Strachunsky L.S., Kozlov S.N. "Penicillins, part 2. Inhibitor-protected and combined penicillins." // Russian Medical Journal, No. 2, 2000 11. Strachunsky L.S., Belousov Yu.B., Kozlov S.N. “Antibacterial therapy. Practical guide." // RC “Pharmedinfo”, 2000.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues
Why don't antibiotics kill coronavirus?
The new Chinese coronavirus negatively affects the respiratory system and leads to the development of pneumonia. It is known that with such lung damage, antibiotics are usually prescribed for treatment. However, in the case of COVID 19, they will not be of any use.
Antibiotics do not kill coronavirus, as they specifically act on the cell membrane of the bacterium. If the patient decides to take the drug independently or administer it in injections for coronavirus infection, then there will be no improvement, but the risk of adverse reactions increases sharply.
The use of amoxicillin for community-acquired pneumonia in children
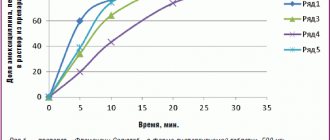
Community-acquired pneumonia (CAP) is one of the most pressing problems of modern medicine and consists of a number of epidemiological, clinical, pharmacological and, finally, social aspects. The paradox of pneumonia is that, on the one hand, impressive results have been achieved in understanding the pathogenesis of the infectious process and increasing the effectiveness of chemotherapy, and on the other hand, there is an increase in the number of patients with severe disease and mortality [3]. Over the course of a year, more than 17 million people are diagnosed with pneumonia in the Russian Federation. The risk group includes children under 5 years of age and elderly people over 65 years of age [4]. Pneumonia is the leading cause of death in children worldwide. Every year, pneumonia claims the lives of about 1 million children under the age of five (in 2015 - 920,136 children, 15% of all child deaths in the world) [1]. In Russia, the incidence of CAP is growing every year. Thus, in 2021, the incidence of community-acquired pneumonia in adults and children was 418.02 per 100 thousand population, which is 24% higher than in the previous 2015 (337.1, respectively) (Fig.).
As in previous years, in 2021, the maximum incidence of CAP was observed in children in the age group of 1–2 years (1456.7 per 100 thousand). The mortality rate from pneumonia in 2021 in the Russian Federation was 4.9 per 100 thousand population, and in some regions it reached 18.8–22.1 per 100 thousand population (in the Altai Republic, Tyumen, Sakhalin, Kirov, Amur regions. ) [19]. According to the Ministry of Health of the Russian Federation, respiratory diseases in children aged 0–17 years occupy third place in the structure of causes of death after external causes and developmental defects. In 2021, the mortality rate of children under 17 years of age from community-acquired pneumonia was 0.4 per 100 thousand population, while over the past 5 years, no significant changes in this indicator have been registered for children under 17 years of age [19].
Community-acquired pneumonia should be understood as an acute disease that arose outside of a hospital or was diagnosed in the first 48 hours from hospitalization, or developed in a patient who was not in nursing homes/long-term medical observation units for more than 14 days, manifested by symptoms of systemic inflammation (fever, shortness of breath, tachycardia, leukocytosis), impaired health (refusal to eat, drowsiness, inappropriate behavior), signs of infectious lesions of the lower respiratory tract (cough, sputum production, chest pain at the height of inspiration) and radiological signs of “fresh” focal infiltrative changes in lungs in the absence of an obvious diagnostic alternative [3].
Pneumonia is an infectious disease associated with the penetration of microorganisms into the respiratory system. The resulting inflammatory reaction in the lung parenchyma depends on the number and virulence of the microorganism, the state of the protective mechanisms of the respiratory tract and the body as a whole. The main route of penetration of the microorganism into the lung tissue is aerogenic. The microorganism, having overcome the protective barriers of the respiratory tract, can enter directly into the alveoli and multiply there intensively. Under the influence of microbial toxins, the permeability of capillaries is disrupted, and serous edema develops. Edema fluid, containing a large number of bacteria, quickly spreads through the alveolar pores to the entire lobe of the lung, often involving the pleura in the inflammatory process. The exudate quickly turns from serous to fibrinous, and the affected part of the lung becomes dense. Impaired bronchial patency, microcirculation disorders, inflammatory infiltration, interstitial edema of the pulmonary parenchyma and decreased airiness of the pulmonary parenchyma lead to impaired gas perfusion and hypoxemia; the latter is accompanied by respiratory acidosis, hypercapnia, compensatory shortness of breath and the appearance of clinical signs of respiratory failure [5].
In accordance with ICD-10 and the “Classification of Clinical Forms of Bronchopulmonary Diseases in Children,” the following forms of pneumonia are distinguished by etiology: bacterial, viral, fungal, parasitic, chlamydial, mycoplasma, mixed [6, 7]. The incidence of bacterial pneumonia in 2021 was 16.5 times higher than viral pneumonia (112.4 and 6.8 per 100 thousand population, respectively).
According to morphological forms, they distinguish: focal, focal-confluent, segmental, polysegmental, lobar and interstitial pneumonia. In the focal form, one or several foci of pneumonic infiltration of 1–2 cm in size occur.
- Focal-confluent (pseudolobar infiltrate) is a heterogeneous massive pneumonic infiltration, consisting of several foci. May be complicated by destructive processes and exudative pleurisy. Segmental - pneumonia, the boundaries of which repeat the anatomical boundaries of the 1st segment.
- Polysegmental - pneumonia, the boundaries of which repeat the anatomical boundaries of several segments. It often occurs with a decrease in the size of the affected area of the lung (atelectatic component).
- Lobar (lobar) pneumonia - the inflammatory process covers a lobe of the lung. A variant of the course of lobar pneumonia is lobar pneumonia.
- Interstitial - along with inhomogeneous infiltrates of the pulmonary parenchyma, there are pronounced, sometimes predominant changes in the interstitium of the lungs. A rare form of pneumonia that develops in patients with immunodeficiency conditions.
According to the flow, CAP is distinguished with an acute course (lasting up to 6 weeks) or protracted (lasting more than 6 weeks). The chronic course of pneumonia is currently not considered and is not included in the “Classification of clinical forms of bronchopulmonary diseases in children” [6, 7].
Based on severity, EP is classified into moderate and severe. The severity of CAP is determined by the severity of clinical manifestations and the presence of complications. Complications: pleural (pleurisy), pulmonary (cavitary formations, abscess), pulmonary-pleural (pneumothorax, pyopneumothorax), infectious-toxic shock [6, 7].
In children 3 months - 5 years old, CAP is most often caused by S. pneumoniae (according to some studies, their share is 70-88% of cases [8, 9]). Of the typical bacteria, H. influenzae type b also plays a role (up to 10% of cases, mainly in children under 2 years of age).
Diagnosis of CAP based on clinical symptoms is associated with significant difficulties. The diagnosis of pneumonia must be made at the patient’s bedside, but it is considered reliable only if infiltration of the lung tissue is detected on a chest x-ray and the presence of at least two of the following criteria [11]:
1) fever above 38 °C for three or more days; 2) cough with sputum; 3) physical symptoms of pneumonia (local weakening of breathing and fine moist rales); 4) leukocytosis > 15 × 109/L and/or the number of band neutrophils > 10%.
To decide on hospitalization and determine the required volume of medical care, it is necessary to assess the severity of CAP. In table Table 2 presents the key criteria for assessing the severity of CAP in children depending on age, proposed by the European Respiratory Society (ERS) [13].
Risk factors for death from pneumonia in children [10]:
- age under 5 years and male gender;
- unfavorable premorbid background of children;
- low socio-economic status of the family;
- late seeking medical help;
- late admission to hospital.
In the vast majority of cases (about 80%), children with CAP can be effectively treated at home. Indications for hospitalization are [11]:
- age up to 6 months of life;
- severe form of the disease;
- the presence of severe underlying diseases - congenital heart disease, chronic lung diseases accompanied by infection (bronchopulmonary dysplasia, cystic fibrosis, bronchiectasis, etc.), immunodeficiency, diabetes mellitus;
- carrying out immunosuppressive therapy;
- lack of conditions for treatment at home or guarantees of implementation of recommendations - socially disadvantaged family, poor social conditions (dormitory, orphanage, temporary accommodation center, etc.);
- lack of response to initial antibiotic therapy (ABT) within 48 hours (maintenance of high fever, increasing respiratory failure, appearance of agitation or depression of consciousness).
ABT has a decisive influence on the prognosis of pneumonia [5, 12]. The choice of ABT in each case of CAP is carried out individually, taking into account the natural activity of the drugs against the pathogen and its possible acquired resistance, the severity and course of the disease, and the presence of contraindications in the patient to the use of certain antibiotics. The principle of choosing ABT depending on the causative agent of CAP is presented in Table. 3.
In clinical practice, especially in outpatient settings, empirical ABT is more often performed, taking into account the most likely pathogen and its sensitivity in the region, the patient’s age, the presence of background diseases, toxicity and tolerability of antibacterial drugs (ABP) for a particular patient.
Evidence-based studies have shown that the use of oral amoxicillin for uncomplicated CAP in children aged 3 months to 5 years is not inferior in effectiveness to benzylpenicillin or ampicillin administered intravenously [15, 16]. In this regard, in all children with CAP who do not have indications for hospitalization, as well as in hospitalized children with moderate CAP, it is advisable to use oral ABT.
In children over 3 months of age, the main antibiotic for the treatment of CAP is amoxicillin (at a standard dose of 45-50 mg/kg per day), since this antibiotic has high, stable activity against the most common and dangerous pathogen - S. pneumoniae, as well as in most cases it is active against H. influenzae [13, 15, 17]. The level of amoxicillin in tissues (including the lungs) is significantly higher than equal doses of phenoxymethylpenicillin and ampicillin. It has a longer half-life, so it is prescribed 2-3 times a day. Food does not affect the bioavailability of amoxicillin, which is important when prescribing to children: unlike oral penicillin, amoxicillin can be given to a child both before and after meals.
When choosing a dosage form, it should be taken into account that the capsule has better bioavailability compared to amoxicillin in tablet form (93% and 70–80%, respectively), which helps to increase efficiency and reduce the risk of adverse events from the intestines.
Amosin® (amoxicillin) is a broad-spectrum antibiotic from the group of semisynthetic penicillins. It disrupts the synthesis of peptidoglycan in the bacterial cell wall during division and growth and causes bacterial lysis. 1–2 hours after administration it reaches maximum concentration in plasma, sputum, bronchial secretions, and pleural fluid. Therapeutic concentrations of amoxicillin are maintained in plasma for 8 hours after oral administration. Amosin® is available in the form of capsules of 250 mg, tablets of 250 and 500 mg and powder for oral suspension of 125, 250 and 500 mg. A new form of Amosin® tablets No. 20 (250 mg) and No. 20 (500 mg) has also appeared. The form of single-dose sachets facilitates the process of preparing the suspension and significantly expands the possibilities of using the drug in children: easy to use (no need to store the prepared suspension in the refrigerator), better It is digestible, allows you to choose the optimal dose depending on body weight and has a pleasant fruity taste. The sachet form is convenient for people with difficulty swallowing.
For children under 5 years of age, Amosin® is prescribed in the form of a suspension. The dose for children under 2 years of age is 20 mg/kg/day in 3 divided doses. For children aged 2 to 5 years, Amosin® is prescribed 125 mg 3 times a day; at the age of 5 to 10 years - 250 mg 3 times a day. Adults and children over 10 years of age weighing more than 40 kg are prescribed 500 mg 3 times a day. The maximum dose for severe manifestation of clinical symptoms is 0.75–1 g 3 times a day.
The sensitivity of S. pneumoniae to amoxicillin remains at a very high level - 99.6%, while the level of resistance to penicillin exceeded the critical value - 10%, to ciprofloxacin and ceftibuten - more than 6%, to cefixime - 5% [14].
For CAP caused by typical bacteria, the duration of therapy is usually 7–10 days, and for atypical bacteria – 10–14 days [13, 15, 17, 18]. ABT can be completed 3–4 days after stable normalization of body temperature [18].
20 children with community-acquired pneumonia aged 5 to 14 years were treated on an outpatient basis in the outpatient department of the State Budgetary Healthcare Institution of the NSO Children's Clinical Hospital No. 6 in Novosibirsk in 2016–2017, of which there were 12 boys (60%) and 8 girls (40%) . Children sought medical help 1–5 days after the onset of pneumonia; on average, the first visit to the doctor took place 2.3 days after the onset of clinical symptoms.
During an objective examination, all children were diagnosed with “community-acquired pneumonia”, of which 18 (90%) had a typical X-ray picture, consisting of focal damage to the lungs, in the remaining 2 children (10%) pneumonia turned out to be X-ray negative, the diagnosis was confirmed by computed tomography data lungs.
The complex of treatment measures included antibacterial therapy with Amosin®, mucolytic agents, physical therapy and therapeutic exercises. Amosin® was used as monotherapy in an age-related dose with a frequency of use 3 times a day according to domestic recommendations for 7–10 days. The average duration of taking Amosin® was 8.3 days. At the same time, stabilization of the clinical condition (effective therapy) was achieved in 90% of children receiving Amosin®. Their clinical symptoms have regressed; children with acute focal pneumonia are not subject to X-ray monitoring, since with positive clinical dynamics, complete resorption of the infiltrate usually occurs after 2–3 weeks. There was no discontinuation of Amosin® due to the development of adverse events.
Thus, the clinical effectiveness of drug therapy, including taking the drug Amosin®, was assessed as recovery in the majority of children diagnosed with community-acquired pneumonia. The above allows us to recommend Amosin® (amoxicillin) for use in outpatient pediatric practice as the drug of choice for acute focal pneumonia.
Literature
- WHO AND UNICEF Bulletins. Electronic resource: https://www.who.int/mediacentre/factsheets/fs331/ru/.
- Vovk E.I., Vertkin A.L. Community-acquired pneumonia at the beginning of the 21st century: the cost of living in a big city // Attending Doctor. 2008. No. 8. pp. 63–65.
- Mustafin T.I., Kudoyarov R.R. Current issues of community-acquired pneumonia // Medical Bulletin of Bashkortostan, 2014. No. 5. P. 39–41.
- World health statistics 2015. World Health Organization 2015. 164 p.
- Community-acquired pneumonia in children. Clinical recommendations, M., 2015. 64 p.
- Geppe N. A., Rozinova N. N., Volkov I. K., Mizernitsky Yu. L. Working classification of the main clinical forms of bronchopulmonary diseases in children. Russian Respiratory Society, 2009. 18 p.
- Geppe N. A., Rozinova N. N., Volkov I. K., Mizernitsky Yu. L. Modern classification of clinical forms of bronchopulmonary diseases in children. // Pediatrics. 2010; 89 (4): 6–15.
- Crawford SE, Daum RS Bacterial pneumonia, lung abscess and empyema/Pediatric respiratory medicine/Ed. Taussig LM, Landau LI Mosby, Inc., 2008: 501–553.
- Tatochenko V.K. Clinical recommendations. Pediatrics (Pneumonia in children) / Ed. A. A. Baranova. M.: GEOTAR-Media, 2005. 28 p.
- Mizernitsky Yu. L., Sorokina E. V., Ermakova I. N. et al. Organization of medical care for children with pneumonia in the Russian Federation // Ros. Vestn. perinatol and pediatrics. 2005; 3:4–8.
- Community-acquired pneumonia in children. Clinical recommendations. M.: Original layout, 2015. 64 p.
- Punpanich W., Groome M., Muhe L. et al. Systematic review on the etiology and antibiotic treatment of pneumonia in human immunodeficiency virus-infected children // Pediatr. Infect. Dis. J. 2011. Vol. 30. No. 10. R. 192–202.
- Esposito S., Patria MF, Tagliabue C. et al. CAP in children/European respiratory monograph 63: Community-acquired pneumonia/Ed. J. Chalmers, M. Pletz, S. Aliberti. 2014. R. 130–139.
- Kozlov R. S. Pneumococci: lessons from the past - a look into the future. Smolensk: MAKMAKH, 2010. 128 p.
- Harris M., Clark J., Coote N. et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011 // Thorax. 2011. Vol. 66, Suppl. 2–23.
- Das RR, Singh M. Treatment of severe community-acquired pneumonia with oral amoxicillin in under-fi ve children in developing countries: a systematic review // PLoS One. 2013. Vol. 25. No. 6. e66232.
- Bradley JS, Byington CL, Shah SS et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America // Clin. Infect. Dis. 2011. Vol. 53. No. 7. e25–76.
- Chuchalin A.G., Sinopalnikov A.I., Kozlov R.S., Tyurin I.E., Rachina S.A. Community-acquired pneumonia in adults: practical recommendations for diagnosis, treatment and prevention: a manual for doctors. M., 2010. 106 p.
- On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2021: State report. M.: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2021. 220 p.
V. V. Provorova1, Candidate of Medical Sciences E. I. Krasnova, Doctor of Medical Sciences, Professor L. M. Panasenko, Doctor of Medical Sciences, Professor V. G. Kuznetsova, Doctor of Medical Sciences, Professor N. G. Paturina, Candidate of Medical Sciences sciences
Federal State Budgetary Educational Institution of Higher Education NSMU Ministry of Health of the Russian Federation, Novosibirsk
1 Contact information
In what cases can antibiotics be prescribed?
Patients who develop pneumonia may be additionally prescribed antibacterial treatment. Drugs are selected based on the severity of the disease, the results of microbiological diagnostics and an analysis of risk factors for encountering microorganisms.
In case of critical condition, drugs with protected aminopenicillins, ceftaroline fosamil, and respiratory fluoroquinolones are prescribed. Beta-lactam antibiotics are prescribed together with macrolides for intravenous administration.
The use of antibiotics without indications or doctor’s recommendations is a direct path to the development of resistance, that is, resistance to this kind of drugs. As a result, if really necessary, the human body simply cannot cope with the bacterial infection and will prolong its course, as well as suffer serious complications.