If a bacterial infection develops, it is imperative to take antibiotics, which are prescribed in a short course for no more than 7 days, so that resistance does not develop. Doctors often recommend Ciprofloxacin or Levofloxacin, but the patient may be intolerant, then they use analogues.
Comparison of the effectiveness of Ciprofloxacin and Levofloxacin
The effectiveness of Ciprofloxacin is quite similar to Levofloxacin - this means that the ability of the drug to provide the maximum possible effect is similar.
For example, if the therapeutic effect of Ciprofloxacin is more pronounced, then using Levofloxacin even in large doses will not achieve this effect.
Also, the speed of therapy - an indicator of the speed of therapeutic action - is approximately the same for Ciprofloxacin and Levofloxacin. And bioavailability, that is, the amount of a drug reaching its site of action in the body, is similar. The higher the bioavailability, the less it will be lost during absorption and use by the body.
What is Levofloxacin?
Levofloxacin is a broad-spectrum antibiotic based on the active substance of the same name. The drug is produced in the form of tablets, injection solution, and eye drops. The following pharmacological action is determined:
- bactericidal effect due to blocking DNA gyrase and topoisomerase 4;
- suppression of bacterial cell DNA synthesis, preventing the formation of a membrane, as a result it dies;
- destruction of gram-positive and gram-negative bacteria, anaerobes.
The drug is indicated for use in infectious and inflammatory diseases. Eliminate bacterial infection of the nasopharynx, respiratory tract, urinary system, skin and soft tissues, and abdominal area. The drug is effective against tuberculosis, but in complex therapy.
The medicine is not approved for use in children, with the exception of complex therapy for cystic fibrosis and pneumonia.
There are many side effects. They arise from the digestive system, cardiovascular and nervous systems, metabolism, sensory organs, musculoskeletal system, urinary system, and immunity. The drug is prohibited for individual intolerance, epilepsy, pregnancy and lactation. Use with caution in old age. Patients are interested in Levofloxacin and alcohol, whether there is compatibility, and what the consequences are. It is prohibited with any drink containing ethyl alcohol.
Comparison of the safety of Ciprofloxacin and Levofloxacin
The safety of a drug includes many factors.
At the same time, with Ciprofloxacin it is quite similar to Levofloxacin. It is important where the drug is metabolized: drugs are excreted from the body either unchanged or in the form of products of their biochemical transformations. Metabolism occurs spontaneously, but most often involves major organs such as the liver, kidneys, lungs, skin, brain and others. When assessing the metabolism of Ciprofloxacin, as well as Levofloxacin, we look at which organ is the metabolizing organ and how critical the effect on it is.
The risk-benefit ratio is when the prescription of a drug is undesirable, but justified under certain conditions and circumstances, with the obligatory observance of caution in use. At the same time, Ciprofloxacin does not have any risks when used, just like Levofloxacin.
Also, when calculating safety, it is taken into account whether only allergic reactions occur or possible dysfunction of the main organs. In other matters, as well as the reversibility of the consequences of the use of Ciprofloxacin and Levofloxacin.
Journal "Diseases and Antibiotics" 2 (2) 2009
Along with β-lactam antibiotics and macrolides, fluoroquinolones are among the most prescribed antimicrobial agents. At the end of the last century, fluoroquinolones with increased antipneumococcal activity appeared on the pharmaceutical market, which since then have often been referred to as “new” or “respiratory” fluoroquinolones. The most successful among them was levofloxacin. In recent years, short courses of high-dose levofloxacin have been used to treat a number of infections. They have been proposed to increase the bactericidal activity of the antibiotic (which depends on its concentration) and reduce the risk of resistance. In the USA, such courses (taking levofloxacin at a dose of 750 mg once a day for 5 days) are officially approved for the treatment of patients aged 18 years and older with community-acquired pneumonia (CAP), acute bacterial sinusitis (ABS), as well as complicated urinary tract infections ( UTI) and acute pyelonephritis (AP) in people with normal renal function (creatinine clearance 50 ml/min). This paper will examine the features and place of levofloxacin and other fluoroquinolones in modern clinical practice.
Historical reference
The first quinolone to find clinical use was nalidixic acid. The drug was discovered during the purification of chloroquine, a substance with antimalarial activity. Nalidixic acid has been used to treat urinary tract infections (UTIs) for more than 40 years. It has moderate activity against a number of gram-negative microorganisms and does not exhibit systemic effects. The introduction of a fluorine atom into the chemical formula of nalidixic acid marked the beginning of a new class of chemical compounds - fluoroquinolones. The first of them, in particular norfloxacin, had a much wider spectrum of activity against gram-negative microorganisms, but, like the prototype drug, did not exhibit a systemic effect. Introduction into clinical practice in the mid-80s. last century, ciprofloxacin and ofloxacin paved the way for the recognition of fluoroquinolones throughout the world. Both drugs showed high activity against not only gram-negative, but also a number of gram-positive, atypical and anaerobic microorganisms. They “brought” fluoroquinolones beyond the narrow framework of “antibiotics for the treatment of UTIs” and laid the foundation for the widespread use of drugs of this class for the treatment of infections of various localizations.
Further evolution of fluoroquinolones was aimed at creating drugs with increased activity against gram-positive bacteria (primarily pneumococci) while maintaining high activity against gram-negative microorganisms [1]. Much attention has been paid to improving the pharmacokinetic properties of drugs. Unfortunately, a number of “new” fluoroquinolones, including such promising ones as trovafloxacin, clinafloxacin, sitafloxacin, are either discontinued or used for very limited indications. The main problem lies in the unacceptable safety profile of these drugs. For the same reason, the use of gatifloxacin was banned in the United States in 2008. In July of the same year, due to the increased risk of adverse drug reactions from the liver, the European Medicines Agency recommended the use of moxifloxacin tablets in patients with CAP only when other antibiotics cannot be used. The lack of a dosage form for parenteral administration and a suboptimal safety profile hinder the widespread introduction of gemifloxacin into clinical practice. Against this background, levofloxacin, which has gained worldwide recognition, really attracts attention.
Attempts to classify fluoroquinolones have been made repeatedly. It was proposed to use the timing of registration of individual drugs, spectrum of action, indications for clinical use and other parameters as a classification criterion. However, there is no generally accepted classification of fluoroquinolones today. Perhaps the most well-known is the division of these antibiotics into “old” and “new”. The first include norfloxacin, pefloxacin, lomefloxacin, ciprofloxacin, ofloxacin, the second - levofloxacin, moxifloxacin, gatifloxacin and gemifloxacin. Another popular approach to classifying fluoroquinolones is to divide them into several generations. In most cases, there are 3 generations of drugs [1–4]; Some authors distinguish subgroups “a” and “b” within generations, and also, depending on the chemical structure, divide antibiotics into “fluoroquinolones” and “naphthyridones” [1]. Significant discrepancies also occur when assigning individual drugs to one generation or another. In some cases, difficulties in classification have objective reasons. For example, levofloxacin is a levorotatory isomer of ofloxacin. From a formal point of view, it should be considered together with ciprofloxacin and ofloxacin. In practice, it is a new generation drug. Levofloxacin has increased activity against pneumococci (and, unlike ciprofloxacin and ofloxacin, is recommended for the treatment of respiratory tract infections), improved pharmacokinetics (and therefore effective when administered once a day) and almost 100% bioavailability when taken orally (which allows carry out step therapy - transfer the patient from an injection form of an antibiotic to an oral one - without any dose adjustment). Finally, levofloxacin appears to be the safest of the fluoroquinolones [5, 6]. For comparison, two other fluoroquinolones with increased antipneumococcal activity, which appeared around the same time as levofloxacin, have either been discontinued (grepafloxacin [1]) or their use has been sharply limited (sparfloxacin).
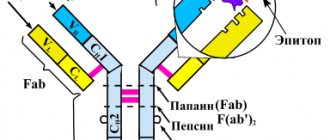
The quinolone structure (Fig. 1) has two six-membered rings in its core containing various radicals. For fluorinated quinolones, the presence of a fluorine atom in the sixth position is fundamental.
Mechanism of action
In a bacterial cell, the targets for the action of fluoroquinolones are the enzymes topoisomerase IV (responsible for organizing the spatial arrangement of the chromosome inside the bacterium and for the separation of chromosomes during cell division) and DNA gyrase (responsible for supercoiling (super-interlacing, “packing”) of bacterial DNA). Each of these enzymes consists of four subunits: DNA gyrase - of two gyrA and two gyrB subunits, which are encoded by the gyrA and gyrB genes, respectively, topoisomerase IV - of two parC and two parE subunits, which are encoded by the parC and parE genes. The region of the polypeptide chain of DNA gyrase or topoisomerase IV in which the binding of fluoroquinolone and the enzyme occurs is called the “quinolone pocket”. In gram-positive bacteria, the main target for the action of levofloxacin is topoisomerase IV, in gram-negative bacteria it is DNA gyrase.
Microbiological activity
Gram-positive bacteria
Levofloxacin exhibits high activity against Streptococcus pneumoniae, both sensitive and resistant (resistant) to penicillin strains. The vast majority of methicillin/oxacillin-susceptible Staphylococcus aureus (MSSA) strains are sensitive to levofloxacin, while among methicillin/oxacillin-resistant (MRSA) strains, no more than 20–25% of isolates remain sensitive to levofloxacin and other fluoroquinolones (Table 1 [7, as amended]).
The activity of the “new” fluoroquinolones against gram-positive bacteria exceeds that of the “old” ones. Usually, to prove the greater activity of a particular drug in vitro, minimum inhibitory concentration (MIC) values are used that are at least 4 times different from those of the reference drug [5]. Although the activity of levofloxacin against pneumococci (regardless of their sensitivity to penicillin) is only 2 times higher than that of ofloxacin and ciprofloxacin, it is within the limits recommended by the American Clinical and Laboratory Standards Institute (CLSI) for treating microorganisms as sensitive to this antibiotic. The increased antipneumococcal activity of levofloxacin allowed the FDA (US Food and Drug Administration) to be the first fluoroquinolone to approve its use in CAP caused by penicillin-resistant pneumococci.
Fluoroquinolones show limited activity against Enterococcus faecalis. Thus, among E. faecalis strains sensitive to vancomycin, only 65% of isolates are sensitive to levofloxacin and 46% to ciprofloxacin.
Streptococcus pyogenes (99.9% of strains) [8, 9] and β-hemolytic streptococci of group A (99.1–100% of strains) [10] retain high sensitivity to levofloxacin, while among coagulase-negative staphylococci the proportion of sensitive isolates is much smaller ( 54.1%) [11].
Gram-negative bacteria
Fluoroquinolones exhibit high activity against common pathogens of respiratory tract infections - Haemophilus influenzae and Moraxella catarrhalis, both non- and β-lactamase-producing strains. The activity of levofloxacin against Escherichia coli is comparable to that of other fluoroquinolones (ciprofloxacin, gatifloxacin). Antibiotics of this class are usually active against Klebsiella pneumoniae, although strains that produce extended-spectrum β-lactamases (ESBLs) often exhibit resistance. The sensitivity of Proteus mirabilis to levofloxacin exceeds 90% and is slightly higher than to other fluoroquinolones. Levofloxacin and other fluoroquinolones are usually highly active against Enterobacter cloacae (Table 1).
Non-fermenting microorganisms are less sensitive to levofloxacin. If the activity of the antibiotic against Pseudomonas aeruginosa (71–94.2% of sensitive strains) and Stenotrophomonas maltophilia (according to the SENTRY study, 86% of sensitive strains) [12] remains quite high, then, for example, among Acinetobacter baumannii strains resistant to ceftazidime , only 19.6% remain sensitive to levofloxacin [13].
Atypical bacteria and anaerobes
Levofloxacin exhibits high activity against Chlamydophila pneumoniae, Legionella pneumophila and Mycoplasma pneumoniae, but has virtually no effect on anaerobes [14].
Resistance
The emergence of resistance to antibiotics of this group is associated with:
1) with a mutation of the DNA gyrase and topoisomerase IV genes localized on the chromosome;
2) activation of active excretion mechanisms (i.e., fluoroquinolones begin to be actively “pumped out” from bacterial cells; this mechanism applies mainly to “old” quinolones).
The basis for the formation of resistance to fluoroquinolones are mutations (amino acid substitutions) in the area between the 67th and 106th amino acid residues in the “quinolone pocket” of sensitive enzymes, which lead to a decrease in their affinity for antibiotics. Depending on at what point in the “quinolone pocket” the amino acid substitution occurred, an increase in the minimum inhibitory concentration of the antibiotic to varying degrees of severity is observed [15].
In the same microorganism, mutations in one or two genes can accumulate, so the formation of resistance is stepwise.
Over the past 10–15 years, there has been a widespread increase in the resistance of clinically significant bacteria to traditionally used antibiotics. However, despite the emergence of resistance to levofloxacin among S. pneumoniae, it remains at a consistently low level (Ј 1%). For example, according to the TRUST study, from 2000 to 2005, resistance of pneumococci to levofloxacin changed from 0 to 0.5%, while to clindamycin over the same period of time it increased 1.5 times (from 12. 1 to 18.6%), and to amoxicillin/clavulanate - 2 times (from 6.5 to 12.9%) [16]. Moreover, if S. pneumoniae showed resistance to two or more antibiotics of different classes (multiple resistance), 99.1% of them remained sensitive to levofloxacin (only 18.3% to cefuroxime, 16.8% to azithromycin) [ 16].
According to large global studies conducted in 1998–2005, all strains of H. influenzae and M. catarrhalis remain sensitive to levofloxacin [7, 9, 17–21]. At the same time, microbiological studies have recorded the emergence and spread of resistance to levofloxacin among E.coli (5.1–15.4%), P.aeruginosa (24.7%), MSSA (3.4–10.1%) and MRSA (76.6–79.2%) [11, 22, 23].
Some features of fluoroquinolones
Interest in this class of antibiotics is explained by the presence of a number of positive properties in fluoroquinolones. Firstly, they, like β-lactams and aminoglycosides and unlike macrolides, have a rapid bactericidal effect against most microorganisms sensitive to them. This circumstance is being given increasing importance due to the growing number of patients with serious diseases, as well as various disorders of the immune system [24]. If bacteriostatic antibiotics (macrolides, tetracyclines, etc.) are suitable for the treatment of mild and moderate infections, then bactericidal antibiotics are suitable for the treatment of diseases of any severity, including the most severe [24].
Secondly, fluoroquinolones, like macrolides and unlike β-lactams and aminoglycosides, exhibit high activity against intracellular pathogens. Atypical microorganisms play a significant role in the etiology of many common infections, in particular CAP. At the same time, they often penetrate and multiply inside macrophages. Pneumococci and Staphylococcus aureus can also survive and multiply inside cells [25]. Therefore, the ability to destroy pathogens located inside the cells of the human body is an important advantage of antibacterial agents.
Fluoroquinolones not only penetrate cells well and are active under specific intracellular conditions, such as low pH. Due to their bactericidal action, they have certain advantages over bacteriostatic antibiotics. This statement can be illustrated by the example of Chlamydophila pneumoniae, an intracellular pathogen that exists in replicative and dormant forms. Fluoroquinolones exhibit high activity against both forms, while bacteriostatic antibiotics are only active against the replicative form [26].
The third feature of fluoroquinolones is their good penetration into organs and tissues. For example, the concentration of β-lactams and aminoglycosides in the tissues of the respiratory tract is 60–70% of their concentration in plasma. The concentrations of fluoroquinolones and macrolides in these tissues significantly exceed plasma concentrations.
The next advantage of fluoroquinolones is the destruction of pathogens with minimal release of various components of bacterial cells. Lipopolysaccharide from gram-negative bacteria has the greatest ability to stimulate the formation of proinflammatory cytokines. The abundant release of this endotoxin from dead bacteria can lead to the development of serious complications, including septic shock. The mechanism of action of fluoroquinolones and aminoglycosides is associated with disruption of the synthesis of DNA and protein, respectively, in the microbial cell. As a result, they cause less endotoxin release than β-lactam antibiotics, which disrupt bacterial cell wall synthesis [26, 27]. Some components of the cell wall of Gram-positive bacteria, such as teichoic and lipoteichoic acids, also induce the formation of proinflammatory cytokines, although the ability to induce their production in Gram-positive microflora is significantly lower than in Gram-negative microorganisms [28]. However, β-lactam antibiotics, which cause extensive disintegration and rupture of bacterial cell walls, result in greater release of these acids than other classes of antimicrobial agents, including fluoroquinolones. In turn, a pronounced effect on the formation of pro-inflammatory cytokines can negatively affect the duration of persistence of disease symptoms [29].
In laboratory conditions, it has been shown that many antibiotics exhibit a post-antibiotic effect and are also capable of suppressing the proliferation of microorganisms at concentrations below the MIC for these pathogens (the so-called subMIC effect). Antimicrobial drugs are dosed so that their concentration at the site of inflammation exceeds the MIC of the probable (or established) pathogen. However, after the antibiotic concentration is reduced below the MIC, bacterial growth and reproduction do not resume immediately. This period of “lag” is called the post-antibiotic effect. For example, the presence of a post-antibiotic effect of levofloxacin has been documented for S. pneumoniae, S. aureus, S. epidermidis, E. coli, E. faecalis, B. fragilis and other microorganisms [30–33], and the duration of the post-antibiotic effect against S .pneumoniae, MRSA, K.pneumoniae, L.pneumophila ranges from 2 to 4.5 hours [14]. The clinical significance of post-antibiotic and subMIC effects remains to be studied, but it appears that they may provide additional theoretical justification for reducing the frequency of antibiotic prescriptions.
Pharmacodynamics of fluoroquinolones
All antibiotics can be divided into dose-dependent and time-dependent. If the antibacterial activity of an antimicrobial drug depends on its concentration at the site of inflammation (so-called dose-dependent antibiotics), then the best effect can be achieved when using high doses of the drug, which are close to toxic [24]. Moreover, the higher the ratio of the maximum (peak) concentration of the antibiotic in plasma to the MIC value of the pathogen, the better. Fluoroquinolones, together with aminoglycosides, amphotericin B and metronidazole, belong to the group of dose-dependent antimicrobial agents.
In recent years, it has been shown that the effectiveness of a dose-dependent antibiotic can be predicted using another pharmacodynamic parameter - the ratio of the area under the pharmacokinetic curve (AUC), which reflects the change in drug concentration over time after its administration, to the MIC (or minimum bactericidal concentration). The numerator often indicates the AUC value for the period of time from the moment of drug administration (zero time period) until the end of the day (AUC24). All other things being equal, the higher the AUC/MIC, the more effective the drug. In studies with fluoroquinolones with increased activity against pneumococci (levofloxacin, gatifloxacin, moxifloxacin, gemifloxacin), it was shown that eradication (extermination) of sensitive gram-positive microorganisms is achieved with an AUC/MIC value of at least 30 [34]. The MIC of levofloxacin for S. pneumoniae is 1 mg/l. In this case, AUC/MIC is equal to 50, i.e. almost 1.7 times higher than the required value for eradication of pneumococci [24]. As for gram-negative microorganisms, their eradication is achieved with an AUC/MIC value of at least 100. All quinolones, starting with the “old” ones, provide an AUC/MIC ratio that far exceeds the minimum requirement.
Monte Carlo simulation studies demonstrated a high probability of achieving target pharmacodynamic parameters against pneumococci when using levofloxacin at a dose of 750 mg once daily (Table 2) [35–37].
Pharmacokinetics of levofloxacin
The bioavailability of levofloxacin in tablets of 500 and 750 mg is » 99% [38].
The drug is almost not metabolized in the liver and is excreted unchanged in the urine. In patients with reduced renal function, dose adjustment is necessary. In patients with liver failure, no dose adjustment is required [38].
Age, sex and racial differences, severe community-acquired bacterial infections do not affect the pharmacokinetics of levofloxacin [38].
Drug-drug interactions
Absorption of levofloxacin in the gastrointestinal tract is reduced when used simultaneously with sucralfate, antacids containing magnesium or aluminum, zinc-containing multivitamins and metal cations (for example, iron). Therefore, at least 2 hours should pass between taking the antibiotic and the listed compounds [38]. No studies of intravenous levofloxacin have examined its interaction when used concomitantly with the listed oral agents. However, single catheter administration of levofloxacin and compounds containing polyvalent cations should be avoided [38].
The use of high-dose short courses of levofloxacin in patients with community-acquired pneumonia
A comparative study of the effectiveness of high-dose short (levofloxacin 750 mg once daily for 5 days) and traditional (levofloxacin 500 mg once daily for 10 days) courses of treatment included 528 patients with CAP of varying severity (classes I –IV on the PSI scale) at the age of 18 years [39]. Patients in the 5-day therapy group received a placebo antibiotic for the next 5 days (i.e., days 6 to 10). The place of treatment of the patient (outpatient, inpatient) was determined by the doctor based on the specific clinical situation and class on the PSI scale. The route of antibiotic administration (orally, intravenously) was also left to the discretion of the attending physician. The primary endpoint of the study was the assessment of clinical effectiveness (cure + improvement) on days 7–14 after completion of treatment. Clinical cure was defined as the disappearance of all symptoms of the disease and the absence of the need for further antibiotic therapy. With clinical improvement, there was a significant decrease in the number and severity of symptoms of the disease, but without their complete elimination; however, continued antibiotic therapy was not required. Clinical failure was defined as lack of response to treatment (or incomplete response) and the need for continued antibiotic therapy.
Microbiological effectiveness was assessed based on the results of cultural examination of samples of respiratory tract secretions or blood. A distinction was made between eradication (disappearance of all pathogens that were isolated when the patient was included in the study), persistence (re-isolation of at least one of the pathogens isolated when the patient was included in the study) and unknown (including patients who, for various reasons, did not submit repeated samples of biological material after completion of the study).
The results of the study are presented in Fig. 2. In terms of clinical and microbiological effectiveness, a high-dose short course of treatment with levofloxacin was not inferior to the traditional one either in the entire population of patients with CAP, or, according to subanalyses, in patients with CAP caused by atypical microorganisms (L.pneumophila, C.pneumoniae and/or M. pneumoniae), in patients with moderate/severe CAP (grades III–IV on the PSI scale), in patients aged ≥ 65 years [39–42]. Moreover, in a post hoc analysis (that is, not planned in advance, but carried out after completion of the study), in patients from the high-dose course group on the 3rd day of treatment, normalization of body temperature and cessation of purulent sputum production were statistically significantly more likely to be recorded (Fig. 3).
There were no significant differences between the compared treatment regimens in the timing of transfer of patients in whom the antibiotic was immediately administered intravenously to oral administration of the drug (Fig. 4).
According to a subanalysis, in patients with CAP caused by atypical microorganisms, the clinical effectiveness of a short high-dose course of levofloxacin was 95.5%, traditional - 96.5% (95% confidence interval -6.8 ... +8.8) [40] . Thus, the high effectiveness of short courses of high-dose levofloxacin has been established in a category of patients who are traditionally recommended to take longer-term antibiotics (up to 14-21 days compared to 7-10 days for CAP caused by typical pathogens - S. pneumoniae, H. influenzae, etc.).
The results of subanalyses in patients with moderate/severe CAP (grades III–IV on the PSI scale) and in patients aged ≥ 65 years are presented in Fig. 5, 6.
The use of high-dose short courses of levofloxacin in patients with acute bacterial sinusitis
A comparative study of the effectiveness of high-dose short (levofloxacin 750 mg once daily for 5 days) and traditional (levofloxacin 500 mg once daily for 10 days) courses of treatment included 780 patients with obstructive heart disease aged > 18 years [ 43]. All patients received oral antibiotics. Patients in the 5-day therapy group received a placebo antibiotic for the next 5 days (i.e., days 6 to 10). During microbiological examination of the material, S. pneumoniae, H. influenzae and S. aureus were most often isolated. The results of the study are presented in Fig. 7.
It has been established that a high-dose short course of levofloxacin in patients with obstructive heart disease is not inferior in effectiveness to the traditional 10-day course. The disadvantages of the study include the late assessment of the effectiveness of the intervention (on the 17th–24th day from the start of treatment). Since patients with ABS have a high rate of spontaneous cure, it is difficult to determine the actual contribution of the antibiotic to achieving cure or improvement [43].
Complicated urinary tract infections and acute pyelonephritis
A comparative study of the effectiveness of a high-dose short course of levofloxacin 750 mg once a day for 5 days and a traditional course of ciprofloxacin 400 mg (if administered intravenously) or 500 mg (if administered orally) 2 times a day for 10 days included 782 patients with complicated UTI (CSI) and 311 patients with AP aged > 18 years [44]. A prerequisite for inclusion was the detection of >105 colony-forming units (CFU) of one or two uropathogens on urine culture. Patients were randomized taking into account the diagnosis (UTI or AP), treatment conditions (outpatient or inpatient) and the presence or absence of a catheter in the urinary tract. The choice of route of antibiotic administration (orally, intravenously) was left to the discretion of the attending physician. The primary end point of the study was the assessment of microbiological effectiveness (pathogen eradication rate) on days 15–22 from the start of treatment.
It was found that a high-dose short course of levofloxacin in patients with UTI and AP is not inferior in effectiveness to the traditional 10-day course of treatment with ciprofloxacin (Fig. 8). In the presence of a catheter in the urinary tract, the frequency of eradication of pathogens was statistically significantly lower than in patients without catheters. Moreover, in patients with catheterized urinary tracts receiving levofloxacin, the frequency of eradication of pathogens was statistically significantly higher than that in patients receiving ciprofloxacin [44].
The results of the study in patients with AP are presented in Fig. 9 [45]. The data obtained did not differ from those in the general group of patients with complicated UTI and AP.
Limitations of the study include the assessment of clinical and microbiological effectiveness at the same time, regardless of the duration of treatment, which could be an argument in favor of preferring a longer course. In addition, mandatory microbiological verification of the etiology of the disease could lead to the inclusion of more severely ill patients in the study, which, in turn, did not exclude an underestimation of the effectiveness of both tested antibiotics [44].
Tolerability of short high-dose levofloxacin regimens
A high-dose short-term treatment regimen with levofloxacin is well tolerated by patients. According to an analysis of the tolerability of high-dose short (1141 people) and traditional (3268 patients) regimens of levofloxacin use in patients with respiratory tract infections, the frequency of adverse drug events (ADEs), which, according to physician researchers, was definitely, possibly or probably associated with taking the antibiotic , did not differ in both groups (8 and 7.6%, respectively). The list and frequency of occurrence of NDEs are presented in Fig. 10. Statistically significant differences in the frequency of development were established only in relation to headache, which, moreover, was recorded very rarely [46].
During treatment with levofloxacin, rare cases of NDEs characteristic of taking fluoroquinolone antibiotics have been described: diarrhea caused by Clostridium difficile; tendon damage; polyneuropathy; hypersensitivity reactions, etc. Although fluoroquinolones are capable of increasing the duration of the QT interval on the electrocardiogram, neither in clinical nor in post-marketing studies of levofloxacin not a single case of torsades de pointes was reported [38, 46]. Phase III studies revealed no differences in the tolerability of levofloxacin in older age groups compared with young and mature patients [38]. The rate of refusal to continue treatment due to the occurrence of AEs associated with taking levofloxacin in patients with respiratory tract infections was 1.5–1.6% [46].
How to use levofloxacin
Intravenous levofloxacin is administered by slow infusion lasting at least 60–90 minutes (depending on the dose). Antibiotic tablets can be taken regardless of food intake. At the same time, liquid dosage forms of levofloxacin for oral administration should be taken 1 hour before or 2 hours after meals. Regardless of the route of administration of the drug, adequate hydration of the body should be ensured to prevent the formation of highly concentrated urine [38].
In patients with impaired renal function receiving levofloxacin at a dose of 750 mg, the dosage is adjusted as follows. When creatinine clearance is 20–49 ml/min, the drug is administered at a dose of 750 mg every 48 hours; with a creatinine clearance of 10–19 ml/min, as well as in patients on hemodialysis or chronic ambulatory peritoneal dialysis, a dose of 750 mg is first administered, then 500 mg every 48 hours.
In patients ≥ 65 years of age, the drug is used with caution in cases of concomitant use of class IA or III antiarrhythmic drugs (risk of QT prolongation) and glucocorticoids (increased risk of tendon damage) [38].
In patients with diabetes mellitus receiving oral hypoglycemic agents or insulin, glycemic levels should be periodically monitored (to avoid hyperglycemia or hypoglycemia with associated symptoms, described with concomitant use of fluoroquinolones, including levofloxacin).
Discussion
The use of short, high-dose courses of levofloxacin not only improves the convenience of treatment, but also reduces the risk of resistance compared with the use of low doses over a longer period of time (for example, 500 mg for 10 days) [47–49].
Distribution of E.coli strains, Klebsiella spp. and other bacteria that produce extended-spectrum blactamases, has limited the use of antibiotics. Most often in such cases, carbapenems (monotherapy) or a combination of fluoroquinolones with aminoglycosides are prescribed. Data on the significance of ESBL production are contradictory. If some publications claim that the clinical effectiveness of antibiotics for infections caused by ESBL-producing and non-ESBL-producing strains of E. coli and Klebsiella spp. does not differ, and ESBL production itself is not an independent risk factor for clinical failure [50], others indicate a significant increase in the cost of treating infections (not UTIs) caused by ESBL-producing E. coli and Klebsiella spp. (mainly due to an increase in the length of stay of patients in hospital) [51]. According to a few and small studies, the activity of levofloxacin against ESBL-producing strains of E. coli and Klebsiella spp. is decreasing, but this issue needs further study [8].
The listed comparative studies of high-dose short course and traditional courses of treatment with levofloxacin were designed to prove that one regimen is not inferior in effectiveness to the other. The results obtained cannot be extended to other nosological forms of diseases. Similarly, the effectiveness of high-dose short-course treatment with levofloxacin compared with other antibiotics used to treat CAP, ABS, complicated by UTI and AP has yet to be established.
Conclusion
Levofloxacin is a fluoroquinolone with increased activity against pneumococci, which, unlike ciprofloxacin and ofloxacin, is recommended for the treatment of respiratory tract infections. It has improved pharmacokinetics (and therefore is effective when administered once a day) and almost 100% bioavailability when taken orally (which allows for step therapy - transferring a patient from an injection form of an antibiotic to an oral one - without any dose adjustment). Levofloxacin has a high safety profile, which distinguishes it from other fluoroquinolones with increased antipneumococcal activity (in 2008, the use of gatifloxacin was discontinued in the United States, and the European Medicines Agency recommended not to use moxifloxacin in tablet form).
In recent years, short courses of treatment with high-dose levofloxacin have been successfully used to treat a number of infections. They have been proposed to increase the bactericidal activity of the antibiotic (which depends on its concentration) and reduce the risk of resistance. In the USA, such courses (taking levofloxacin at a dose of 750 mg once a day for 5 days) are officially approved for the treatment of patients > 18 years of age with community-acquired pneumonia, acute bacterial sinusitis, as well as complicated urinary tract infections and acute pyelonephritis in people with normal renal function (creatinine clearance > 50 ml/min).
The clinical and microbiological effectiveness of short high-dose courses of levofloxacin for these diseases has been demonstrated in comparative studies with a traditional (10-day) course of treatment with levofloxacin (for community-acquired pneumonia and acute bacterial sinusitis) and ciprofloxacin in standard dosages (for complicated urinary tract infections and acute pyelonephritis). At the same time, in patients with community-acquired pneumonia from the high-dose course group, on the 3rd day of treatment, normalization of body temperature and cessation of purulent sputum production were statistically significantly more likely to be recorded.
The introduction into clinical practice of short, high-dose courses of levofloxacin for the above respiratory and urinary tract infections will help improve the convenience and effectiveness of treatment and reduce the risk of resistance selection during treatment.
Comparison of addiction between Ciprofloxacin and Levofloxacin
Like safety, addiction also involves many factors that must be considered when evaluating a drug.
So, the totality of the values of such parameters as “syndrome o” for Levofloxacin is less than the similar values for Ciprofloxacin. Withdrawal syndrome is a pathological condition that occurs after the cessation of intake of addictive or dependent substances into the body. And resistance is understood as initial immunity to a drug; in this it differs from addiction, when immunity to a drug develops over a certain period of time. The presence of resistance can only be stated if an attempt has been made to increase the dose of the drug to the maximum possible.
Efficacy of treatment with analogues
Ciprofloxacin and Levofloxacin are high-quality antibacterial agents. They are used for infectious and inflammatory pathologies. With the correct course of application and dosage, a quick effect occurs. If there are contraindications for use, it is better to buy analogues.
The therapeutic effect of analogues is observed in the case of using the drug prescribed by a doctor. Only he knows what is better to use, Amoxiclav, Sumamed or Azithromycin. It is advisable to first carry out a bacteriological culture of the separated organ (for example, the nasopharynx) in order to know which active substance will affect the body, eliminating the infection.
If the condition continues to worsen, the drug may have been prescribed incorrectly. It is recommended to conduct a general blood and urine test to determine the condition of the body. Thanks to the selection of analogues, doctors will be able to continue treating infectious pathologies, even if the first medicine did not lead to positive dynamics. Improvements are evidenced by a decrease in body temperature, appearance of appetite, elimination of pain and redness, and body activity. Before choosing a substitute, look at whether the drug is approved during pregnancy, lactation, and childhood.
Comparison of side effects of Ciprofloxacin and Levofloxacin
Side effects or adverse events are any adverse medical event that occurs in a subject after administration of a drug.
Levofloxacin has more adverse effects than Ciprofloxacin. This implies that the frequency of their occurrence is low with Levofloxacin and low with Ciprofloxacin. Frequency of occurrence is an indicator of how many cases of an undesirable effect from treatment are possible and registered. The undesirable effect on the body, the strength of influence and the toxic effect of drugs are different: how quickly the body recovers after taking it and whether it recovers at all. When using Levofloxacin, the body's ability to recover faster is higher than that of Ciprofloxacin.
Characteristics of Ciprofloxacin
Ciprofloxacin is a broad-spectrum antibiotic. Its price is not expensive, but its effectiveness is high. It is based on the active substance of the same name, which causes the following pharmacological action:
- suppression of bacterial DNA gyrase;
- disruption of DNA synthesis, which prevents the growth and reproduction of bacterial cells;
- bactericidal effect on gram-negative and gram-positive microorganisms;
- low toxicity to the human body and its tissues.
The drug is produced in injections for intravenous infusion, tablets, and eye drops. Therefore, the drug is suitable for the treatment of many diseases. It is recommended to use it for infectious and inflammatory pathologies of the following parts of the body:
- upper and lower respiratory tract;
- organs of vision;
- urinary system, genitals;
- circulatory system during the development of sepsis;
- digestive tract;
- nasopharynx.
Ciprofloxacin is one of the latest generation antibiotics. It is allowed to be used by both adults and children. Its effectiveness is high, so it is possible to treat even such pathologies as sepsis, anthrax, cystic fibrosis (in complex therapy). There are many side effects, they occur in almost every system of the body. Therefore, the drug is used only under the supervision of a doctor in limited dosages.
Comparison of ease of use of Ciprofloxacin and Levofloxacin
This includes dose selection taking into account various conditions and frequency of doses. At the same time, it is important not to forget about the release form of the drug; it is also important to take it into account when making an assessment.
The ease of use of Ciprofloxacin is approximately the same as Levofloxacin. However, they are not convenient enough to use.
The drug ratings were compiled by experienced pharmacists who studied international research. The report is generated automatically.
Last update date: 2021-01-10 10:02:00