Muscle relaxants are medications that relax the human striated muscles. Muscle relaxants are drugs that reduce the tone of skeletal muscles, thereby reducing a person’s motor activity, up to complete immobilization. Until a certain time, they were widely used exclusively in anesthesiological practice to relieve muscle tone during operations. Today, the scope of use of muscle relaxants in medicine and aesthetic cosmetology has expanded significantly.
What are muscle relaxants?
Osteochondrosis is almost always accompanied by acute pain, which hampers movement and prevents normal movement and simple physical actions. Therefore, the patient is prescribed drugs that can reduce muscle tone, reduce pain, and increase the effectiveness of physiotherapeutic procedures. They are recommended for use against the background of manual therapy and exercise therapy; the dosage is selected individually, after undergoing a full examination.
There are two types of muscle relaxants:
- Antispasmodics. Aimed at reducing muscle tone. Helps relax and bring muscles back to normal. They are used in case of severe spasms or moderate intensity.
- Blockers. They help to quickly relax muscles and relieve nervous tension. Moreover, with their help, the “zero mark” is achieved. Used exclusively in surgery.
Muscle relaxants are manufactured by pharmaceutical companies and are based on glycerin or benzimidazole. But there are also mixed varieties, such as, for example, “Belofen”, “Mydocalm”.
Muscle relaxants for osteochondrosis are used only when mobility is lost or reduced; they are not suitable for relaxing muscles and eliminating pain. These medications are not used independently, but are often included in a complex and perfectly complement anti-inflammatory medications, painkillers and antibiotics.
Types of muscle relaxants
Based on the mechanism of action, there are two main types of muscle relaxants:
Central muscle relaxants are drugs that inhibit the central structures of muscle tone. These chemicals have a direct effect on the parts of the central nervous system, brain and spinal cord that are involved in the regulation of muscle tone. Peripheral muscle relaxants are agents that penetrate into direct neuromuscular transmission. These medications relax voluntary muscles by blocking the signal from the motor nerve to the muscle.
How do pills relax muscles?
Medicines that can relax muscle tissue are prescribed for many diseases. Most often these are neuralgia, sciatica, osteochondrosis, bruxism, coxarthrosis and others. With their help, skeletal muscles are immobilized and their reflex activity is stopped. The substance included in the drug acts directly on the nervous system, thereby regulating muscle tone. The use of non-steroidal anti-inflammatory drugs simultaneously with muscle relaxants enhances their effect.
The main features of the presented medications are:
Ointments for cervical osteochondrosis
- selective action;
- decreased muscle excitability in the affected area;
- good tolerability of drugs due to well-thought-out composition;
- long-lasting and high efficiency;
- does not reduce the patient’s ability to work or general activity;
- They combine well with other medications and are included in almost any therapeutic program.
Muscle relaxants for osteochondrosis are the basis of therapy, since without them the effectiveness of physiotherapy or therapeutic exercises decreases, and the effectiveness of all tactics is generally lower. But independent use of medications is excluded, since their use must be carried out in a hospital setting under the supervision of a specialist. Each drug has its own indications and contraindications, age restrictions, and inadmissibility of use with a number of substances.
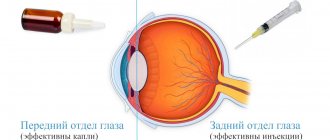
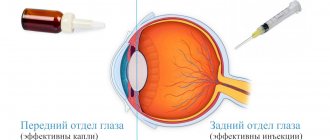
For your information! The therapeutic effect of muscle relaxants in tablets is not high enough, so in severe cases, intramuscular administration of the drugs is prescribed.
Muscle relaxants are used in tablets and injections, the form is selected by the doctor individually
The action of muscle relaxants.
With diseases of the spine such as spondyloarthrosis, osteochondrosis, spondyloarthritis, nerve impulses pass through the affected segments along the spinal cord, causing neuromuscular tension, as a result of which people suffering from spinal diseases are deprived of motor activity, while experiencing pain. In addition, severe pain forces a person with spinal diseases to take a forced position of the body, which potentiates spasm and pain. Only the action of muscle relaxants can change such a pathological process. Muscle relaxants that enter the systemic circulation reach the spinal cord, where they have a stimulating effect on certain groups of receptors, which in turn counteract the release of individual amino acids into the bloodstream, which inhibits the transmission of nerve impulses through nerve cells and endings. This action of muscle relaxants
allows you to reduce muscle tone, causing them to relax.
According to their action, muscle relaxants are divided into different groups, used not only for diseases of the spine and back. There are two main types of muscle relaxants: peripheral action (used for muscle paralysis due to tetanus and convulsions) and central action (reduce the transfer of nervous excitation in the fibers of the central nervous system without causing muscle immobilization).
Contraindications and side effects
Drugs that relax muscles are prescribed when patients experience severe pain (cutting, pulling, aching), even at rest, radicular syndrome, sudden muscle wedge when bending over or sneezing, neuralgic disorders. The list of symptoms is quite wide, and when to use this particular group of medications is decided by the doctor at his own discretion.
You cannot buy medications at your own discretion, since, in addition to benefits, they can also cause harm to the body. They should be prescribed by a doctor, based on the tests obtained and after studying the patient’s medical history. Their use is unacceptable in the presence of the following pathologies:
- kidney failure or liver disease;
- regular drug use or alcohol addiction;
- mental disorders;
- epilepsy or Parkinson's disease;
- tendency to neurasthenia or psychosis;
- increased seizure activity;
- ulcerative colitis and gastrointestinal pathologies.
Drugs that relax the muscle structure are not prescribed during pregnancy or while breastfeeding. If you violate the order of administration or use drugs with contraindications, unwanted side effects may develop. Most often, patients complain of general weakness, severe headache, depression of consciousness, surges in blood pressure, heart rhythm disturbances, depression or insomnia. There may also be problems with the digestive tract.
Muscle relaxants for cervical osteochondrosis
Osteochondrosis is a pathological condition that causes reflex muscle strain. Therefore, it is impossible to do without the use of muscle relaxants, especially if its localization is the neck and shoulder girdle. They are used in combination with chondroprotectors, painkillers, and anti-inflammatory drugs. The following drugs relieve stiffness in cervical osteochondrosis well:
- "Baclofen."
- "Mydocalm."
- "Tizanidine."
- "Sirdalud".
It is recommended to use them within 5-7 days from the moment of severe neck pain. The tablet form is great for adults; teenagers are often prescribed injections for better effects. In addition to them, drug therapy includes ointments and patches with an irritating effect.
In surgery, muscle relaxants are used as injections and completely block the muscles, eliminating any tension, even reflex.
List of drugs
Muscle relaxants are prescribed by the attending physician, taking into account the patient’s age, pain intensity and concomitant diseases. Therefore, you cannot use the same remedies that were effective for a neighbor or relative. The pharmaceutical market today offers a wide variety of options. The presented list of drugs that relax the muscle structure is provided for information.
"Mydocalm"
It is one of the safest means used for muscle relaxation in osteochondrosis. It can be found on the market under the name "Tolperisone". Its distinctive feature is the reduction of muscle tissue spasm, the provision of a small antispasmodic effect, as well as adrenergic blocking and antispastic effects. The drug is prescribed in small dosages, and if the body tolerates it well, then it is gradually increased.
The main features of the medicine are:
- Lack of sedation, which allows you to drive a vehicle.
- Available in the form of tablets or injections.
- Not for use on children under 3 years of age.
- Low likelihood of developing an allergic reaction.
The medicine is well tolerated by people of any age, and thanks to it it is possible to reduce the amount of non-steroidal anti-inflammatory drugs taken. It contains lidocaine, which additionally numbs the affected area.
"Sirdalud"
Another representative of the group of muscle relaxant drugs that are used for osteochondrosis to relieve muscle spasms. It is prescribed in a small dosage, which is gradually increased if there is no negative reaction from the body. The range of applications for this medication is wider than the previous one, since doctors also use it in cases of amputation, convulsive syndrome or cerebral palsy. Its appointment is not allowed if the following points are present:
- liver diseases;
- renal failure;
- individual intolerance to individual components;
- during the period of taking drugs such as Ciprofloxacin, Fluvoxamine;
- children under 18 years of age.
The drug is taken exclusively under the supervision of a specialist, since if the dosage is incorrect, it can cause a number of unwanted side effects.
Unlike other drugs, Sirdalud is offered by manufacturers only in tablets
"Baclofen"
The presented drug is suitable for long-term use due to the fact that it is easily tolerated. Prescribed to patients over 14 years of age in the form of injections. It combines well with other drugs, but during the treatment process it is necessary to strictly monitor your health status through testing. The daily dosage for an adult is 100 mg.
"Tizanidine"
Developed and used specifically for the treatment of cervical osteochondrosis. Thanks to its thoughtful composition, the drug reduces pain, eliminates stiffness of movement, increases the effectiveness of prescribed physiotherapy procedures and the patient’s overall quality of life.
The likelihood of side effects occurring is minimal only if there have been violations of the dosage regimen or the recommended dose has been exceeded without permission. In other cases, the drugs are well tolerated and cope well with the task.
The listed names of drugs are offered in the form of tablets and injections; ointments can be found less frequently. They, in turn, are the safest way to treat osteochondrosis. Medicines are taken according to the doctor’s recommendation and the established rules in the instructions. You should not combine the drug with medications sold in pharmacies without a prescription, unless approved by your doctor. In addition, you should not increase or decrease the dosage on your own, as this always leads to undesirable consequences.
Exceeding the concentration of muscle relaxants in the body causes vomiting, disturbances in perception of the world, headache, loss of consciousness or coma. The active substance affects the central nervous system, so the consequences of an overdose are always unpleasant.
The place of natural herbal NSAIDs in the treatment of nonspecific chronic back pain
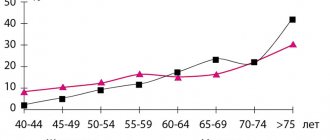
Pain in the lower back is not only a neurological, but also a general medical problem, since its development can be based on a variety of causes, which are conventionally divided into vertebrogenic and non-vertebrogenic. Among the vertebrogenic causes of back pain are protrusion of the intervertebral disc, osteophytes, instability of the spinal motion segment, subluxations, arthrosis, vertebral fracture, osteoporosis, osteoarthritis, vertebral tumors. Pain syndrome of non-vertebrogenic origin is associated with reflex muscle tension in response to painful impulses, which is the physiological basis for the creation of a “muscle corset” that immobilizes the damaged area. With prolonged tension, the muscle itself becomes a source of pain. Nonvertebrogenic back pain includes myofascial pain syndromes, referred pain in diseases of internal organs, psychogenic pain, pain in spinal tumors, etc. [12,14,15]. Based on the fact that in 8–10% of patients back pain is secondary, when managing patients with chronic nonspecific back pain, a differential diagnosis is made with specific causes of back pain. It is necessary to remember about the “red flags” - symptoms of a possible specific cause of pain, namely: • the onset of persistent back pain before the age of 15 years or after 50 years; • non-mechanical nature of the pain (pain does not decrease at rest, in a lying position, in certain positions); • gradual increase in the severity of pain; • history of cancer; • development of pain against the background of fever, loss of body weight; • complaints of prolonged stiffness in the morning; • symptoms of spinal cord damage; • changes in urine, blood or other laboratory tests [5]. The International Society for the Study of Spondyloarthritis also identified clinical criteria for chronic back pain of inflammatory origin [45]: 1. Reduction of pain with moderate physical activity 2. Increased pain at night 3. Gradual development 4. Age of onset over 40 years 5. No reduction intensity of pain at rest The high prevalence of pain syndromes in the lower back causes an increase in the need for effective painkillers. According to an analysis of the pharmaceutical market conducted by the independent research center ROMIR in 2001, the most popular drugs purchased by more than 58% of the population are over-the-counter analgesics, with 25% purchasing analgesics once a week or more often. 17.3% of patients take analgesics for back pain [13]. The results of numerous randomized controlled trials convincingly show that the most effective drugs for chronic back pain are nonsteroidal anti-inflammatory drugs (NSAIDs). A meta-analysis of 65 controlled studies showed that NSAIDs in general and selective COX-2 (cyclooxygenase-2) inhibitors, including those, are significantly effective for acute back pain or exacerbation of chronic pain without radicular syndrome [26,34,40]. No significant difference was found between the effectiveness of the most commonly used NSAIDs and COX-2 inhibitors, however, COX-2 differs for the better in terms of safety, although in some studies there is evidence of the negative impact of these drugs on the cardiovascular system [9,40]. In clinical guidelines for the diagnosis, treatment and prevention of nonspecific pain in the lower back, compiled by the Association of Rheumatologists of Russia and the Russian Interregional Society for the Study of Pain, NSAIDs and COX-2 inhibitors are considered first-line drugs for chronic nonspecific back pain, but attention is drawn to the high the frequency of side effects with long-term use of these drugs [6]. For chronic nonspecific back pain, it is recommended to use non-injectable forms of NSAIDs ahead of the development of pain (taken by the hour, and not as the pain intensifies). When choosing a drug, a stepwise approach should be used from a high dose of a weaker drug to a low dose of a stronger drug [6]. To treat chronic back pain, drugs from other groups are also used - antidepressants, anticonvulsants with analgesic effects, muscle relaxants, pepper patch applications, opiate-containing drugs. It should be noted that antidepressants, anticonvulsants with an analgesic effect and opiate-containing drugs are especially indicated for the development of neuropathic pain, as well as in the presence of concomitant emotional and affective disorders. Since psychological factors play an undoubted role in the development of chronic back pain, therefore, non-pharmacological treatment methods, primarily psychotherapy, are also effective in such patients [1,11]. The effectiveness of NSAIDs for chronic back pain is due not only to analgesic, but also anti-inflammatory effects. Therefore, NSAIDs are the drugs of choice in the treatment of chronic back pain of inflammatory origin (for example, spondyloarthritis). However, the effectiveness of NSAIDs has also been noted for chronic nonspecific back pain. With the advent of new high-resolution diagnostic methods, it has been shown that patients with nonspecific chronic back pain have structural changes in connective tissue [31]. At the same time, the presence of signs of degenerative-dystrophic damage to spinal tissues in patients with nonspecific chronic back pain does not correlate with either the nature of the pain or its intensity [8]. A number of studies have revealed markers of inflammation in the tissues of the lumbar region in patients with chronic nonspecific back pain: high activity of C-reactive protein [39], increased levels of interleukin-6 (IL-6) [21], tumor necrosis factor (TNF) [36 ]. In patients with chronic back pain, compared to patients with acute radiculopathy, the number of macrophages in the connective tissue structures is increased [27], which is also a marker of chronic inflammation. There is a point of view that the maintenance of chronic pain is largely due to ongoing peripheral sensitization caused by inflammatory changes [37]. One experimental study showed that during inflammatory processes in the periphery, there is an increase in the level of COX-2 in the dorsal horn of the spinal cord, which leads to the phenomenon of neuronal hyperexcitability and the development of neuropathic pain [42]. This hypothesis is confirmed by the effectiveness of NSAIDs for chronic back pain, which was shown in a meta-analysis that included more than 60 controlled studies [22]. One study [2] compared the effectiveness of NSAIDs for acute and chronic back pain. It was found that NSAIDs for chronic back pain (as opposed to acute) reduce only the pain syndrome, but not emotional and affective disorders, which also indicates the significant role of the phenomenon of peripheral sensitization in the maintenance of chronic pain. The main disadvantage of traditional NSAIDs is the existence of restrictions on their long-term use, which are due to the presence of side effects, primarily from the gastrointestinal tract. COX-2 inhibitors have a lesser effect on the gastrointestinal tract, but the question of the cardiac safety of these drugs remains open. In addition, 2–4% of the population has intolerance to NSAIDs, manifested by allergic reactions in the form of respiratory disorders and skin rashes [24]. The development of NSAID intolerance syndrome is associated with the fact that inhibition of COX-1 reduces the production of prostaglandin E2, which normally suppresses the production of sulfidoleukotrienes and other mast cell mediators [24]. Among the adverse drug reactions associated with long-term use of NSAIDs, along with gastrointestinal disorders, one can also note hemorrhagic syndrome, the development of bronchospasm, tocolytic effect, necrospermia, as well as nephro-, hepato- and hematotoxicity [41]. Poor drug tolerance largely determines the active use of complementary and alternative treatment methods by patients with chronic back pain. Thus, a study was conducted in the USA that included more than 23 thousand patients with various neurological pathologies. It has been shown that more than 50% of patients with chronic back pain regularly use complementary and alternative therapies [47]. The leading reason for the use of complementary and alternative treatments is the ineffectiveness or intolerance of traditional pharmacotherapy, while the adherence of patients with chronic back pain to alternative and complementary research methods is extremely high [28]. An alternative to NSAIDs in patients with chronic back pain may be the use of herbal preparations with analgesic and anti-inflammatory effects [4]. Extracts of harpagophytum, willow bark, nettle, avocado seed, rose hips, boswellia and ginger have NSAID properties, and these plants have been used in folk medicine for many centuries. Ginger rhizome extract is used in Ayurvedic and Tibetan medicine as an anti-inflammatory and analgesic [25]. The active ingredients of the extract are gingerols and diarylheptanoids. In recent years, the official drug Zinaxin, based on ginger extract, has become available. Zinaxin has a number of unique pharmacological properties [16]: firstly, the drug contains two specially selected ginger extracts with a proven synergistic effect - Alpinia galanga (galangal) and Zingiber officinale (ginger). Ginger extracts have critical bioavailability, so the second feature of Zinaxin is the unique technology for the production of the dosage form - lipocap, which allows increasing bioavailability by 34%. Lipocap technology is the presence in the dosage form of a shell of diacetates of simple diglycerides, which are stable at low pH, which protects the biocomplex (ginger extracts and lipocap) from exposure to the aggressive environment of the stomach [16]. In the intestine, under the influence of bile, lipocap forms lipid micelles, the core of which is ginger extract. Absorption occurs in the small intestine by passive absorption upon contact of lipid micelles with the cell membrane of the cilia of the intestinal epithelium, from where the drug is transported into the lymphatic vessel, then into the thoracic lymphatic duct and enters the bloodstream, bypassing the liver [16]. Thus, the required therapeutic concentration of the drug is quickly created in the blood. The mechanism of action of ginger extract is associated with the inhibition of COX-2 and 5-lipoxygenase (LOX), which, in turn, leads to a decrease in the formation of prostaglandins, prostacyclins, thromboxane and leukotrienes [46]. Unlike most non-selective NSAIDs, ginger extract does not inhibit COX-1 and, therefore, is free from unwanted drug reactions associated with its blockade [35,48]. In addition, ginger extract can suppress the synthesis of pro-inflammatory cytokines IL-1β and TNF-α [25,30], as well as stimulate the synthesis of anti-inflammatory IL-4 and IL-10 [29]. One of the most interesting works where the pharmacological effect of ginger extract was shown is the study by Lindmark L. et al. [32]. Synoviocyte culture samples (synovial tissue obtained from patients suffering from osteoarthritis during surgery) were placed in either ginger extract or indifferent medium. Inhibition of COX-2 and TNF-α was observed in 100% of synoviocyte culture samples placed in ginger extract [32]. It is assumed that the direct target of the effect of ginger extract is the regulation of the expression of the genes TNF-α, IL-1β, IL-6, IL-8 and IL-10 through the influence on the nuclear transcription factor NF-κB [25,33]. In addition, ginger extract suppresses the expression of chemokines that induce the transport of macrophages to the inflammation zone [23,38]. The effectiveness of ginger extract for chronic pain may be due to several mechanisms. First, blockade of COX-2 in the dorsal horn of the spinal cord may prevent the development of neuropathic pain [42]. One study showed that ginger extract suppresses both acute and chronic inflammation, and its effect is associated not only with inhibition of prostaglandin synthesis, but also with a decrease in the production of nitric oxide and calcitonin-related peptide gene, the most important components of the development of neurogenic inflammation [ 44]. Moreover, ginger extract, like capsaicin, has the properties of an antagonist of both TPRV and ankyrin TPRA receptors, therefore, it can be effective for neuropathic pain, especially when it is burning in nature [19,23]. Fundamental research into the analgesic and anti-inflammatory effects of ginger gave rise to the active use of the drug in traditional clinical practice, and since 2001, a number of clinical studies have been conducted that meet the requirements of evidence-based medicine. A randomized, double-blind, placebo-controlled, parallel, multicenter (10 centers in the USA) study of the effectiveness of Zinaxin (at a dose of 2 capsules per day) included 261 patients with osteoarthritis for 6 weeks [18]. Pain intensity was assessed using a visual analogue scale (VAS), and stiffness was assessed using the WOMAC scale. A significant analgesic effect was noted by the second week of taking the extract, and the most pronounced effect was observed by the 6th week, while the severity of pain in the Zinaxin group was 40% less than in the placebo group (p = 0.005). Already by the second week of taking Zinaxin, stiffness decreased, and the most pronounced significant effect was noted in the 6th week of treatment (difference from placebo by 31%, p = 0.018). In the second part of the study, the analgesic activity of ginger extract was compared with the selective COX-2 blocker celecoxib at different doses (100 and 200 mg). Pain intensity was assessed using VAS. The analgesic effect of celecoxib developed rapidly by the end of the 2nd week of administration, while the effect of ginger extract increased gradually. However, from the 2nd to the 6th week of observation, the effectiveness of celecoxib and ginger extract did not differ significantly, while both drugs were significantly superior to the effects of placebo [18]. The analgesic effect and safety of Zinaxin in the treatment of chronic pain syndrome in osteoarthritis were studied in detail in a study by V.N. Drozdov. [3]. 27 patients received Zinaxin (2 capsules per day), 31 patients received diclofenac at a dose of 100 mg/day. Over the course of 6 months of observation, positive dynamics were noted both in the Zinaxin group and in the diclofenac group, while no significant differences were obtained between the groups (Fig. 1). In addition, the study measured the concentration of prostaglandins E2 and E12 in the gastric mucosa. It was shown that in patients taking diclofenac, the level of prostaglandins E2 and E12 decreased significantly by the 21st day of administration, while in patients taking Zinaxin, the level of prostaglandins did not change. Among patients taking diclofenac, side effects from the gastrointestinal tract were observed in 42% after 3 weeks of use and in 81% after 6 months of use. In the Zinaxin group, side effects from the gastrointestinal tract were observed in 4% after 3 weeks of use and in 4% after 6 months of use. 16% of patients taking diclofenac had to stop taking it after 3 weeks due to gastroenterological side effects; after 6 months, 42% of patients stopped treatment with diclofenac. In the Zinaxin group, not a single patient stopped taking the drug due to side effects. Thus, the effectiveness of Zinaxin with long-term use was comparable to the effectiveness of diclofenac, while Zinaxin was significantly superior to diclofenac in tolerability. Another randomized, double-blind, placebo-controlled study examined the effectiveness of Zinaxin in the complex treatment of pain in osteoarthritis [17]. A significant positive effect was revealed in relation to the main manifestations of the disease: pain, stiffness, and decreased daily activity. The combined use of ginger extract and traditional NSAIDs made it possible to halve the doses of the latter and, accordingly, reduce the severity of side effects. Since chronic nonspecific back pain is one of the main reasons for the constant use of NSAIDs, a study was conducted on the effectiveness of motor therapy with ginger extract and combined treatment with ginger extract and ibuprofen, which included 175 patients with chronic nonspecific back pain. It was shown that in a group of combined treatment with ginger extract and Ibuprofen, a reliable decrease in pain occurs in the 1st week, while in a group of patients who received monotherapy with ginger extract - only in the 2nd week. Nevertheless, starting from the third week and over the next 7 weeks of observation, the effectiveness of combined treatment with ginger extract and ibuprofen and monotherapy with ginger extract was stable and did not significantly differ. Consequently, when selecting the treatment scheme for patients with chronic non -specific back pain, it is possible to recommend the appointment of traditional NSAIDs in a short course with the subsequent long -term use of ginger extract drugs [43]. Preparations based on ginger extract can be recommended to patients with muscle pain associated with physical activity. Black CD CJSC. [20] conducted a randomized dual blind, a placebo -controlled study, which included 74 healthy volunteers. For 11 days, the studied volunteers received significant physical activity in the form of sports exercises, while 34 people received ginger extract, and 40 - a placebo. According to the results of the study in a group that received an active drug, the intensity of pain and the severity of painful muscle tension was reliably lower on the 3rd day [20]. Therefore, the drug can also be used for episodes of muscle pain associated with physical activity (for example, work on a garden area) or a long stay in an uncomfortable position (for example, working at a computer). Thus, despite the fact that ginger has been used in medicine for many centuries, official approved products containing extracts of this plant have become available recently. The appearance of such drugs has become an alternative to the use of traditional NSAIDs: it is proved that drugs containing ginger extract (Zinaxin) with prolonged use in effectiveness are no worse than traditional NSAIDs, but significantly exceed the latter in safety. The high efficiency of the natural drug is largely due to the technology of its production, which allows you to quickly achieve the necessary therapeutic concentration in the blood. Zinaxin is successfully used by rheumatologists to treat chronic pain in osteoarthritis. The use of Zinaxin in patients with pain syndromes in neurological practice also seems promising. Zinaxin complies with the requirements of the standards for the management of patients with non -specific pain in the lower part of the back, compiled by the Association of Rheumatologists of Russia and the Russian Interregional Society for the Study of Pain, where preference is given to non -injection forms of NSAIDs, taking ahead of the development of pain, as well as a steppe approach from a high dose of a weaker to a low dose of a stronger means. The first data on the effectiveness and safety of the drug for the treatment of chronic non -specific back pain and muscle pain associated with physical exertion were obtained. The possibility of using zinaxine for other pain syndromes, for example, in chronic headaches, for the preventive treatment of migraine, with neuropathic pain, requires further study.
Literature 1. Voznesenskaya T.G. Pain in the back and limbs // In the book: Pain syndromes in neurological practice / A.M. Wayne et al. – M: MEDpress, 1999. – pp. 217–284. 2. Voznesenskaya T.G. Back pain: a neurologist's view. // Consilium medicum. – 2006. – No. 8. – p.28–32. 3. Drozdov V.N. Zinaxin is a new safe drug for the treatment of osteoarthritis. // RMJ. – 2008. – No. 1. – p.1–3. 4. Zyryanov S.K., Nelga O.N., Belousov Yu.B. Pain therapy: how to reduce the risk of developing adverse side effects // Handbook of a polyclinic doctor. - 2007. - No. 7. - pp. 14–16. 5. Kukushkin M.L. Pathophysiological mechanisms of pain syndromes // Pain – 2003. – No. 1. – P. 5–12. 6. Nonspecific pain in the lower back. Diagnosis, treatment, prevention. // M.KomplektServis. – 2008. – 70 p. 7. Parfenov V.A. Diagnosis and treatment for back pain. // RMJ. – 2004. – No. 12. – p.115–118. 8. Podchufarova E.V. Pain in the lumbosacral region: diagnosis, treatment. // RMJ. – 2006. – No. 2. – p.12–19. 9. Podchufarova E.V. Back pain: evidence-based medicine and clinical practice. // Difficult patient. – 2010. – No. 3. – p.14–21. 10. Podchufarova E.V., Yakhno N.N. Backache. // M.: Geotar Medicine. – 2010. – 368 p. 11. Podchufarova E.V., Yakhno N.N., Alekseev V.V. and others. Chronic pain syndromes of lumbosacral localization: the significance of structural musculoskeletal disorders and psychological factors. // Pain. – 2003. – No. 1. – p.38-43. 12. Popelyansky Ya.Yu. Orthopedic neurology. – T.2. – Kazan, 1997. – 487 P. 13. Tabeeva G.R. Nurofen in the treatment of neurogenic pain syndromes. // Consilium-medicum. – 2006. – No. 3. – p.32–37. 14. Travell D.G., Simons D.G. Myofascial pain. – M.: Medicine, 1989. – T.1–2. 15. Khabirov F.A. Clinical neurology of the spine. – Kazan, 2002. – 472 P. 16. Shikh E.V., Eremenko N.N. Drugs of natural origin as an alternative way of treating pain syndrome in rheumatology. // Issues of modern pediatrics. – 2008. – No. 1. – p.64–66. 17. Yakimenko E.A., Zakatova L.V., Kravchuk O.E. and others. Study of the effectiveness and safety of the use of zinaxin in the complex therapy of patients with osteoarthritis // Ukrainian Therapeutic Journal. - 2005. - No. 1. - P. 64–67. 18. Altman RD, Marcussen KC Effects of a ginger extract on knee pain in patients with osteoarthritis // Arthritis Rheum. - 2001. - v. 44. - R. 2531–2538. 19. Bandell M, Story GM, Hwang SW, et al. Noxious cold ion channel TRPA1 is activated by pungent compounds and bradykinin. //Neuron. – 2004. – v.41. – p.849–857. 20. Black CD, Herring MP, Hurley DJ, et al. Ginger (Zingiber officinale) Reduces Muscle Pain Caused by Eccentric Exercise. // J Pain. – 2010. – in print. 21. Burke JG, Watson RW, McCormack D, et al. Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators. // J Bone Joint Surg Br. – 2002. – v.84. – p.196–201. 22. Chou R., Huffman LH Medications for acute and chronic low back pain: a review of the evidence for an American pain society/American college of physicians clinical practice guideline. // Ann Intern Med. – 2007. – v.147. – p.505–514. 23. Chrubasik JE, Roufogalis BD, Chrubasik S. Evidence of effectiveness of herbal antiinflammatory drugs in the treatment of painful osteoarthritis and chronic low back pain. // Phytother Res. – 2007. – v.21. – p.675–683. 24. De Weck AL, Sanz ML, Gamboa PM, et al. Nonsteroidal anti–inflammatory drug hypersensitivity syndrome. A multicenter study. I. Clinical findings and in vitro diagnosis. // J Investig Allergol Clin Immunol. – 2009. – v.19. – p.355–369. 25. Frondosa CG, Sohrabi A., Polotsky A., et al. An in vitro screening assay for inhibitors of proinflammatory mediators in herbal extracts using human synoviocyte cultures. // In Vitro Cell. Dev. Biol. – Animal. – 2004. – v.40. – p.95–101. 26. Haroutiunian S., Drennan DA, Lipman AG Topical NSAID therapy for musculoskeletal pain. // Pain Medicine. – 2010. – v.11. – p.535–549. 27. Heavner JE, Bosscher HA, Wachtel MS Cell types obtained from the epidural space of patients with low back pain/radiculopathy. // Pain Pract. – 2009. – v.9. – p.167–172. 28. Kanodia AK, Legedza AT, Davis RB, et al. Perceived benefit of Complementary and Alternative Medicine (CAM) for back pain: a national survey. // J Am Board Fam Med. –2010. – v.23. – p.354–362. 29. Kim SO, Chun KS, Kundu JK, et al. Inhibitory effects of [6]–gingerol on PMA–induced COX–2 expression and activation of NF–kappaB and p38 MAPK in mouse skin. // Biofactors. – 2004. – v.21. – p.27–31. 30. Kiuchi F., Iwakami S., Shibuya M., et al. Inhibition of prostaglandin and leukotriene biosynthesis by gingerols and diarylheptanoids. // Chem Pharm Bull. – 1992. – v.40. – p. 387–391. 31. Langevin HM, Stevens–Tuttle D, Fox JR, et al. Ultrasound evidence of altered lumbar connective tissue structure in human subjects with chronic low back pain. // BMC Musculoskeletal Disord. – 2009. – v.3. – p.151. 32. Lindmark L., Sohrabi A., Phan PV, et al. Modulation of pro–inflammatory mediator and metalloproteinase expression in human synoviocytes. // Materials of the 5th symposium of ICRS. – 2004. – p.93–97. 33. Lindsley HB, Smith DD, Cohic CB, et al. Proinflammatory cytokines increase human synoviocyte expression of functional intercellular adhesion molecule–1 (ICAM–1). // Clin Immunol Immunopathol. – 1993. – v.68. – p.331–320. 34. Machado LAC, Kamper SJ, Herbert RD, et al. Analgesic effects of treatments for non–specific low back pain: a meta–analysis of placebo–controlled randomized trials. // Rheumatology. – 2009. – v.48. – p.520–527. 35. Nurtjahja–Tjendraputra E, Ammit AJ, et al. Effective anti–platelet and COX–1 enzyme inhibitors from pungent constituents of ginger. // Thromb Res. – 2003. – v.111. – p.259–265. 36. Ohtori S., Inoue G., Ito T., et al. Tumor necrosis factor–immunoreactive cells and PGP 9.5–immunoreactive nerve fibers in vertebral endplates of patient with discogenic low back pain and modic type 1 or type 2 changes on MRI. // Spine. – 2006. – v.31. – 1026–1031. 37. Omoigui S. The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3 – inflammatory profile of pain syndromes. // Med Hypotheses. – 2007. – v.69. – p.1169–1178. 38. Phan PV, Sohrabi A, et al. Ginger extract components suppress induction of chemokine expression in human synoviocytes. // The Journal of Alternative and Complementary Medicine. – 2005. – v.11. – p.149–154. 39. Rannou F., Ouanes W., Boutron I., et al. High-sensitivity C-reactive protein in chronic low back pain with vertebral end-plate Modic signal changes. // Arthritis Rheum. – 2007. – v.57. – p.1311–1315. 40. Roelofs PD, Deyo RA, Koes BW, et al. Nonsteroidal anti–inflammatory drugs for low back pain: an updated Cochrane review. // Spine. – 2008. – v.33. – p.1766–1774. 41. Roumie CL, Arbogast PG, Mitchel EFJr., et al. Prescriptions for chronic high-dose cyclooxygenase-2 inhibitors are often inappropriate and potentially dangerous. // J Gen Intern Med. – 2005. – v.20. – p.879–883. 42. Seybold VS, Jia YP, Abrahams LG Cyclooxygenase-2 contributes to central sensitization in rats with peripheral inflammation. // Pain. – 2003. – v.105. – p.47–55. 43. Shikh E. Open comparative study in patients with osteoarthritis of the knee stages I–III: all patients with NSAIDs intolerance. // / 44. Shimoda H., Shan SJ, Tanaka J., et al. Anti–inflammatory properties of red ginger (Zingiber officinale var. Rubra) extract and suppression of nitric oxide production by its constituents. // J Med Food. – 2010. – v.13. – p.156–162. 45. Sieper J., van der Heijde D., Landewe R., et al. New criteria for inflammatory back pain in patients with chronic back pain: a real patient exercise by experts from the Assessment of SpondyloArthritis international Society (ASAS). // Ann Rheum Dis. – 2009. – v.68. – p.784–788. 46. Tjendraputra E, Tran VH, Liu-Brennan D, et al. Effect of ginger constituents and synthetic analogues on cyclooxygenase–2 enzyme in intact cells. // Bioorg Chem. – 2001. – v.29. – p.156–163. 47. Wells RE, Phillips RS, Schachter SC, et al. Complementary and alternative medicine use among US adults with common neurological conditions. // J Neurol. – 2010. – in print. 48. Wu H, Ye DJ, Zhao YZ, et al. Effect of different preparations of ginger on blood coagulation time in mice. // Zhongguo Zhon Yao Za Zhi. – 1993. – v.18. – p.147–149.